
II. Definitions
- Nausea
- Urge to vomit, "sick to Stomach" or "queasy"
- Vomiting (Emesis)
- Forcible expulsion of Stomach contents
- Retching
- Spasms of respiratory Muscle activity before Emesis
- Regurgitation
- Passive retrograde flow of esophageal contents
- Rumination
- Chewing and Swallowing of regurgitated food
- Dry Heaves (non-productive Vomiting)
- Retching without expulsion of any gastric contents
- Projectile Vomiting
- Forceful Emesis without preceding Nausea
- Associated with Increased Intracranial Pressure
- Acute Nausea and Vomiting
- Nausea and Vomiting for <7 days
- Chronic Nausea and Vomiting
- Nausea and Vomiting persisting longer than one month
- Hematemesis
- See Upper Gastrointestinal Bleeding
- Vomiting of fresh blood (suggests acute or severe Upper Gastrointestinal Bleeding)
- Coffee-ground Emesis
- See Upper Gastrointestinal Bleeding
- Vomiting of black blood (altered by gastric acid)
- Stercoraceous Vomiting or Fecal Vomiting
- Vomiting of fecal material (due to obstruction)
- Bilious Emesis
- Vomiting of bile stained (green) fluid
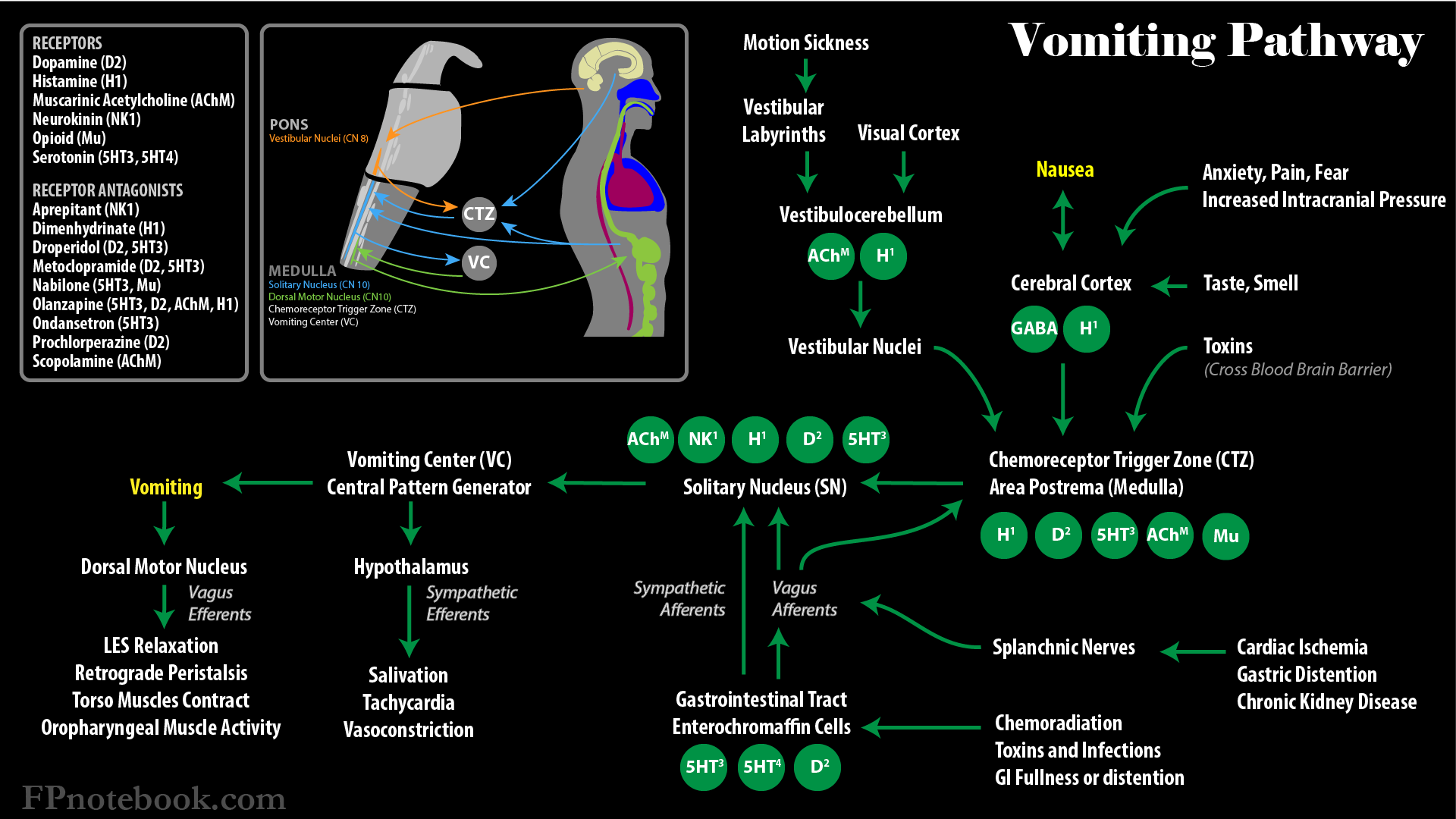
III. Pathophysiology
- Nausea usually precedes Vomiting
- Physiologic Control of Vomiting
- Lateral reticular formation in Medulla
- Chemical stimulation via ChemoreceptorTrigger Zone
- Vomiting is of Involuntary mechanism
- Glottis closes
- Diaphragm contracted and fixed
- Pylorus closes
- Gastric wall and esophageal orifice relaxes
- Abdominal Muscles contract forcefully
- Associated physiologic events
- Ptyalism (Excessive Salivation)
- Tachycardia (occurs with nauses)
- Bradycardia (occurs with Retching)
- Defecation (may accompany Vomiting)
- Images
IV. Causes
- See Vomiting Causes
- See Vomiting Causes in Children
- See Vomiting in Pregnancy (Morning Sickness)
- See Vomiting in Cancer
- See Psychogenic Vomiting
- See Medication Induced Vomiting
- Most Common Causes
- Acute Gastroenteritis
- Vomiting should be followed by Diarrhea
- Medication Induced Vomiting
- Acute Gastroenteritis
V. History
- See Vomiting History for Clinical Clues
- Systemic Symptoms and Signs
- Emesis Characteristics
- Timing between food and Emesis
- Emesis appearance
- Undigested food or milk or yellow color (Stomach contents)
- Hematemesis (Upper GI Bleeding)
- Bilious Emesis (Small Bowel Obstruction)
- Gastrointestinal Symptoms or Signs
- Abdominal Pain before Vomiting (red flag)
- Signs of Gastrointestinal Bleeding
- Hematemesis
- Melana
- Heartburn or indigestion
- Dysphagia
- Constipation
- Diarrhea
- Diarrhea that follows Vomiting is consistent with Gastroenteritis
- Vomiting that follows Diarrhea is consistent with enteritis (or Urinary Tract Infection in girls, women)
- Jaundice
- Genitourinary Symptoms
- Urine Output
- At least three times daily in infants and twice daily in children and adults
- Dysuria
- Urgency or frequency
- Hematuria
- Urine Output
- Neurologic Symptoms and Signs
- Altered Level of Consciousness (GCS, mental status)
- Focal neurologic deficits
- Papilledema
VI. Exam
- Observe for Dehydration
- Weight loss since prior exam
- Decreased skin turgur
- Dry mucus membranes (or not making tears in children)
- Sinus Tachycardia
- Orthostatic Hypotension
- Decreased Capillary Refill
- Other systemic signs of serious illness
- Abdominal examination
- Abdominal Distention
- Abdominal wall Hernia
- Peritoneal signs (abdominal guarding, Rebound Tenderness)
- Abdominal Trauma (e.g. Bruising)
- Abdominal tenderness to palpation
- Epigastric Pain: Gastric Ulcer
- Right upper quadrant pain: Cholecystitis
- Right lower quadrant pain: Appendicitis (esp. with Psoas Sign, Rosving's sign)
- Flank Pain: Pyelonephritis or Uretolithiasis
- Bowel sounds
- Hyperactive suggests Gastroenteritis
- High pitched suggests Small Bowel Obstruction
- Absent or decreased suggests ileus
- Other significant findings
- Hepatomegaly
- Splenomegaly
- Abdominal mass
- Ascites
- Genitourinary exam
- Inguinal Hernia
- Testicular Torsion (testicular tenderness, swelling, absent Cremasteric Reflex)
- Ovarian Torsion
-
Neurologic Examination
- Nystagmus (Acute Vestibular Syndrome)
- Papilledema
- Focal neurologic deficits
- Peripheral Neuropathy
- Cerebellar exam (coordination and gait testing)
- Altered Level of Consciousness
- Skin
VII. Differential Diagnosis
- See Vomiting Causes
- See Upper Gastrointestinal Bleeding
- Ptyalism (Excessive Salivation)
- Gastroesophageal Reflux Disease (Acid Reflux)
- Forceful Coughing
- Post-nasal drainage
- Asthma, Bronchitis or Bronchiolitis
- Pneumonia
- Undigested Food Regurgitation
- Esophageal Obstruction
- Esophageal Diverticulum
- Overfilled Stomach
- Delayed Gastric Emptying or Gastroparesis
VIII. Labs
- Complete Blood Count
- Serum Electrolytes (e.g. Chem8 or SMA-7)
- Liver Function Tests
- Serum Lipase
- Erythrocyte Sedimentation Rate
- Urinalysis
- Urine Pregnancy Test
- Consider endocrine conditions
- Consider serum drug levels of current medications
- Consider stool studies for concurrent Diarrhea
- Consider cardiac evaluation
IX. Imaging (as clinically directed)
- Abdominal Flat and Upright XRay Indications
- Signs or symptoms of mechanical obstruction
- Small Bowel Obstruction
- Gastric outlet obstruction
-
Abdominal CT with oral and IV Contrast
- Detection of Intestinal Obstruction or abdominal mass
- Right upper quadrant Ultrasound
- Suspected Cholecystitis
- Pancreatitis
-
Chest XRay
- Detection of abdominal free air
- Head Imaging (CT Head or MRI Head)
- Indicated to evaluation for Intracranial Mass
- Consider in Projectile Vomiting, Vomiting without Nausea, morning Vomiting or neurologic changes
X. Diagnostics
- Upper endoscopy
- Most sensitive for mucosal lesions
- Gastric Emptying Study (Evaluates for Gastroparesis)
- Ingestion of radiolabeled meal
- Electrogastrography (Abnormal gastric emptying)
- Electrodes placed on abdominal skin over antrum
- Antroduodenal Manometry
- Measures intraluminal pressure over time
- Upper GI with Small Bowel follow through
- Evaluation of function (e.g. Gastroparesis)
- Double-contrast barium studies are more accurate
XI. Management
- See Vomited Medications
- Symptomatic control of Vomiting
- Management of Dehydration and Electrolyte loss
XII. Management: Persistent Unexplained Vomiting
- Complete history, physical, diagnostics completed
- Consider dysmotility evaluation
- Consider possible Gastroparesis causes
- Consider empiric prokinetic
- Consider functional causes or Psychogenic Vomiting
- Consider longterm symptomatic therapy
XIII. Complications
XIV. References
- (2017) Crit Dec Emerg Med 31(4): 19-25
- (1988) Dorland's Medical Dictionary, Saunders, p. 1848
- Feldman (1998) Sleisenger Gastrointestinal, p. 117-126
- Friedman (1991) Medical Diagnosis, Little Brown, p. 174
- Heilenbach in Marx (2002) Rosen's Emergency Med, p. 178
- Anderson (2013) Am Fam Physician 88(6): 371-9 [PubMed]
- Quigley (2001) Gastroenterology 120(1):263-86 [PubMed]
- Scorza (2007) Am Fam Physician 76:76-84 [PubMed]