
II. Definitions
- Supraventricular Tachycardia
- Rapid heart rhythms originating in the atrium or Atrioventricular Node
- Transmit via the Bundle of His and result in rapid ventricular response
III. Causes: Narrow Complex Tachycardia (Mnemonic: 5H 4T PS) Triggers
- See Paroxysmal Supraventricular Tachycardia (PSVT)
- Similar list to Reversible Causes of Cardiopulmonary Arrest (5H5T)
- Hypoxemia
- Hypovolemia
- Hyperthermia
- Hyperkalemia or Hypokalemia
- Hyperthyroidism
- Tamponade (Cardiac Tamponade)
- Tension Pneumothorax
- Toxins, medications and drugs
- Caffeine
- Tobacco
- Alcohol
- Cannabinoids
- Pseudophedrine (or other Sympathomimetics)
- Methamphetamine
- Bronchodilators
- Inotropes
- Antipsychotics
- Thrombus
- Pain, Exercise or Stress
- Structural abnormalities
- Congenital Heart Disease (especially in children)
- Hypertrophic Cardiomyopathy
- Infiltrative Cardiomyopathy (e.g. Sarcoidosis, Tuberculosis)
- Electrical Disorders (e.g. Prolonged QT Syndrome, WPW)
- Prior Atrial Surgery
IV. Types: Narrow Complex Tachycardia
- Sinus Tachycardia
- Supraventricular Tachycardia
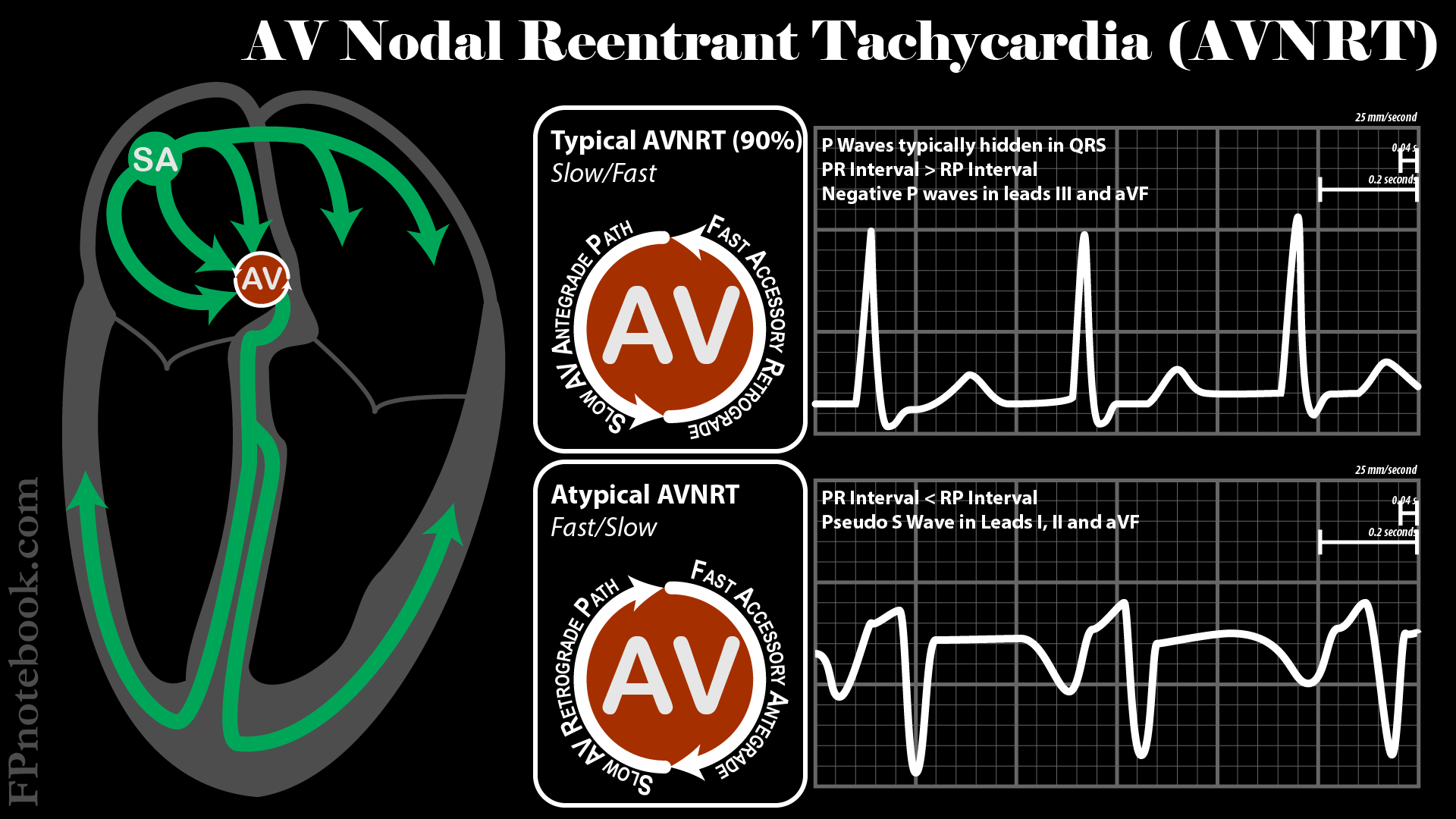
- Atrioventricular Nodal Reentry (AVNRT)
- Signal down the slow AV nodal pathway and retrograde up the fast AV nodal pathway
- In 10% of cases, the signal reentry route is reversed
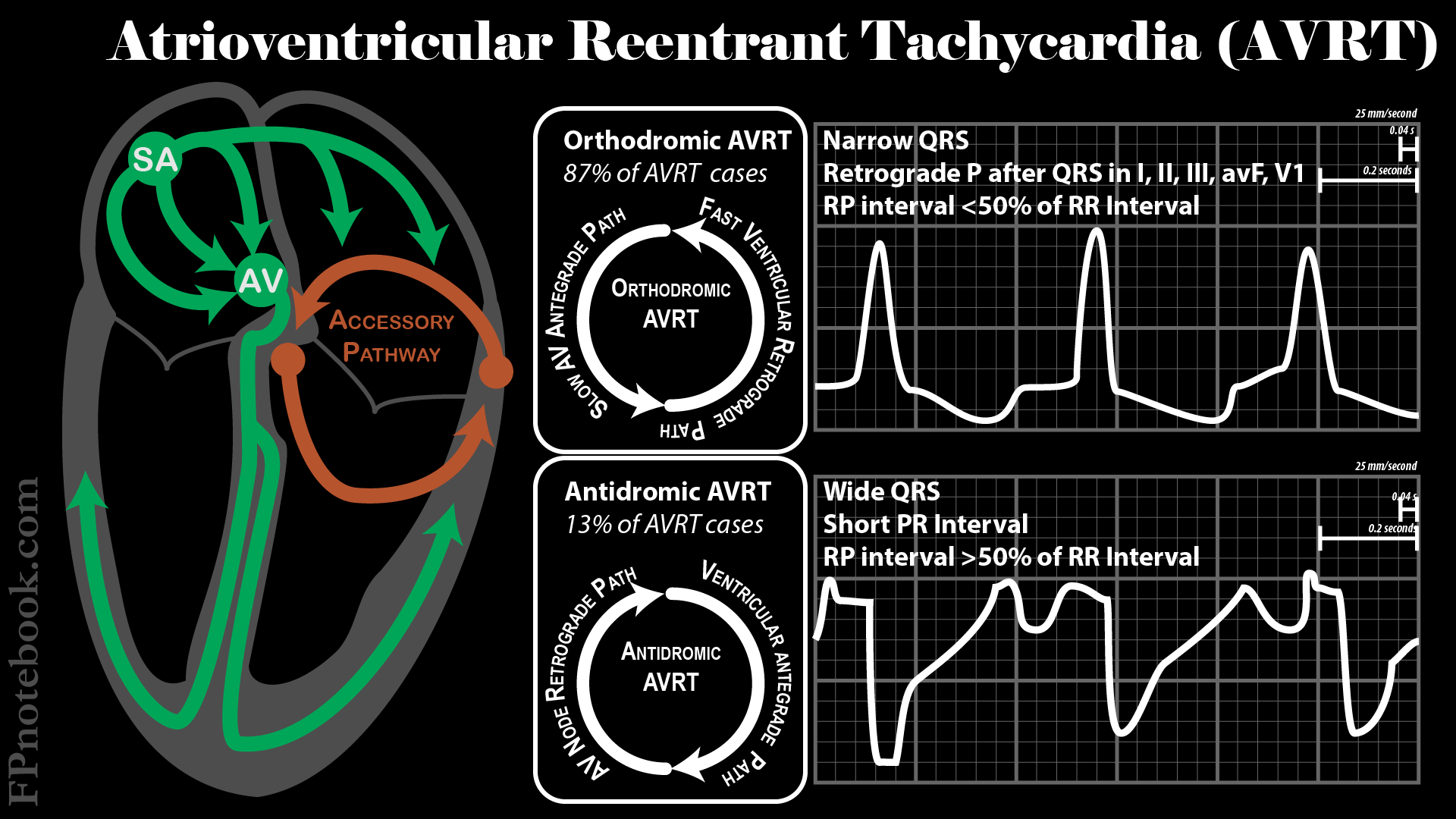
- Atrioventricular Reciprocating Tachycardia (AVRT)
- Includes Wolff-Parkinson-White Syndrome (characterized by delta wave)
- Accessory pathway outside the AV Node
- Atrial Tachycardia (AT)
- Junctional Ectopic Tachycardia
- Atrioventricular Nodal Reentry (AVNRT)
- Other Atrial Tachycardias with rapid ventricular response
V. Differential Diagnosis: Adults - Narrow Complex Tachycardia (key question is 'regular or irregular')
- Sinus Tachycardia (regular)
- Irregular Supraventricular Tachycardia (may also present as wide complex if aberrancy)
- Regular Supraventricular Tachycardia
- Atrial Flutter
- Atrioventricular Nodal Reentry (AVNRT): 60% of SVT cases (esp. women)
- Atrioventricular Reciprocating Tachycardia (AVRT): 30% of SVT cases
- Atrial Tachycardia (AT): 10% of SVT cases
- Junctional Ectopic Tachycardia
- Secondary causes (very high Heart Rates >220-240, refractory or recurrent tachydysrythmia)
VI. Differential Diagnosis: Children - Narrow Complex Tachycardia
- Common
- Orthodromic Atrioventricular Reciprocating Tachycardia (Orthodromic AVRT, or ORT)
- Most common in children (typical, narrow complex SVT)
- Atrioventricular Nodal Reentry (AVNRT)
- Second most common SVT in children (but rare in young children)
- Orthodromic Atrioventricular Reciprocating Tachycardia (Orthodromic AVRT, or ORT)
- Uncommon
- Ectopic Atrial Tachycardia
- Similar to sinus rhythm except for altered P Wave appearance and more rapid rate
- Atrial Flutter (uncommon in children outside the newborn period)
- Atrial Fibrillation (very rare in children)
- Ectopic Atrial Tachycardia
-
Congenital Heart Disease (CHD) history
- CHD predisposes patients to scarring with risk of reentrant pathways
- Intra-atrial reentrant Tachycardia (IART)
- Appears similar to Atrial Flutter
- Typically treated with rate control on Diltiazem (if over age 2-5 years), followed by cardioversion
VII. History
- Timing
- Rapid onset and resolution
- Supraventricular Tachycardia
- Slow onset and resolution
- Rapid onset and resolution
- Precipitating factors
- Caffeine or stimulants, stress (see triggers above)
- Supraventricular Tachycardia or Sinus Tachycardia
- Cardiovascular disease or onset with activity
- Caffeine or stimulants, stress (see triggers above)
VIII. Symptoms
- Common
- Severe
- Altered Mental Status
- Chest pressure, tightness or Angina
- Diaphoresis
- Syncope or Presyncope
IX. Exam
- Thyromegaly (Hyperthyroidism, Thyroiditis)
- Cardiovascular
- Tachycardia (regular or irregular rhythm)
- Cardiac Murmur (valvular heart disease)
- Friction Rub (Pericarditis)
- Third Heart Sound (CHF)
X. Signs: Electrocardiogram
-
Sinus Tachycardia
- P Waves present and normal
- Variable R-R with constant PR Interval
- Heart Rate varies with activity
- Rate lower than PSVT
- Infants < 220 (may approach this with fever)
- Children < 180
- Adults < 160
- Supraventricular Tachycardia
- P Waves absent or abnormal
- Fixed Heart Rate (constant R-R)
- Abrupt rate change
- Rate higher than Sinus Tachycardia (especially if Heart Rate twice normal for age or higher)
- Infants > 220
- Children > 180
- Adults > 160
- Very high rates >220-240 suggests underlying secondary cause (e.g. Thyrotoxicosis, see above)
XI. Labs: General
- Precautions
- Paroxysmal Supraventricular Tachycardia does not require routine labs in many cases (esp. known prior history of PSVT)
- Patients who are asymptomatic after PSVT resolves, and without underlying other risks need not undergo laboratory testing
- Initial tests to consider
- Thyroid Stimulating Hormone (TSH)
- Basic metabolic panel
- Complete Blood Count
- Chest XRay
- Additional tests to consider (in adults)
- Ambulatory EKG Monitoring (e.g. Zio Monitor, Holter Monitor or Event Monitor)
- Additional tests to consider for concerns of underlying Cardiomyopathy
XII. Labs: Troponin
- Background
- No lab testing is indicated in routine PSVT that resolves without symptoms
- Repeat EKG and reevaluate patient history and exam 15 minutes after return to sinus rhythm
- Asymptomatic patients with normal ekg and exam after return to sinus rhythm need no further testing
- Consider lab testing driven by specific positive symptoms, signs or risk factors after return to sinus rhythm
- Serum Troponin Is NOT typically indicated in Supraventricular Tachycardia (SVT)
- SVT is rarely due to acute occlusive Myocardial Infarction
- ST Depression is commonly seen as a stress response to Tachycardia, but is not indicative of a coronary event
- Serum Troponin Is often elevated in SVT (esp. if prolonged) but is not associated with 90 day adverse outcomes
- Despite low efficacy and resulting Cascades of Care, Troponin Is obtained in 80% of ED SVT evaluations (abnormal in 30% of cases)
-
Troponin Indications
- Persistent concerning EKG changes after conversion to sinus rhythm
- Symptoms and signs specifically suggestive of underlying Acute Coronary Syndrome (not attributable to SVT alone)
- References
- Mattu and Swaminathan (2022) EM:Rap 22(12): 7-8
XIII. Management: Stable Patients
- New emphasis on use of one Antiarrhythmic
- Contrast to prior Antiarrhythmic soups
- Pro-arrhythmic effects increase with poly-drugs
- Supraventricular Tachycardia Management in the Adult
- Supraventricular Tachycardia Management in the Child
XIV. Management: Unstable Patients
XV. Management: Cardiology Consultation Indications
- Uncertain diagnosis or management
- Recurrent Supraventricular Tachycardia refractory to medications
- High risk profession or activity (e.g. truck driver, airline pilot, rock climbing, Scuba Diving)
- Ablation considered over medication (patient preference)
- Wolff-Parkinson-White Syndrome (characterized by delta wave) or other preexcitation
- Structural heart disease (e.g. Hypertrophic Cardiomyopathy)
- Syncope associated with Supraventricular Tachycardia
- Wide complex QRS on EKG
XVI. References
- Claudius, Behar and Bar Cohen in Herbert (2014) EM:Rap 14(5):1-2
- Hebbar (2002) Am Fam Physician 65(12):2479-86 [PubMed]
- Helton (2015) Am Fam Physician 92(9): 793-800 [PubMed]
- Nasir (2023) Am Fam Physician 107(6): 631-41 [PubMed]
- Cardiopulmonary Resuscitation Guidelines