
II. Definitions
- Syncope
- Rapid onset of transient loss of consciousness
- Inability to maintain postural tone
- May be associated with a fall
- Resolves spontaneously and quickly without intervention
- Presyncope (Near-Syncope)
- Weakness, Dizziness, Light Headedness or "graying out" of consciousness without loss of postural tone
- Evaluate Presyncope with the same vigor as Syncope
- Presyncope has the same risks of adverse event as Syncope
- Grossman (2012) Am J Emerg Med 30(1): 203-6 +PMID:21185670 [PubMed]
III. Epidemiology
- Up to one third of Syncope cases are idiopathic
- Common diagnosis
- Occurs in up to 40-50% of adults, and 75% over age 75
- Accounts for 1 to 1.5% of ER visits and up to 6% of admissions (250,000 admissions annually)
IV. Precautions
- Careful history (including from bystanders), exam, and ekg should direct limited diagnostics and disposition
- Always consider serious cause differential diagnosis (see rule of 15s below)
- Near-Syncope should be evaluated with the same thoroughness as Syncope (causes are the same)
V. Pathophysiology
- Decreased global cerebral perfusion (usually on standing)
- Two key mechanisms
- Systemic vasodilation (Reflex Mediated Syncope)
- Decreased Cardiac Output (Cardiac Syncope, Orthostasis)
VI. Risk Factors
- Elderly
- Structural heart disease (e.g. Aortic Stenosis)
- Congestive Heart Failure
- Coronary Artery Disease
VII. Causes: Neural or Reflex Mediated Syncope (no Cardiovascular Risk, most common in all ages, 45% of cases)
- Vasovagal Syncope (Vasodepressor Syncope)
-
Situational Syncope
- Micturition Syncope or with Defecation
- Cough Syncope (or sneezing)
- Valsalva (brass instrument playing, weight lifting)
- Hyperventilation
- Carotid Sinus Syncope
- Glossopharyngeal neuralgia (uncommon)
- Syncope occurs with Swallowing, talking, sneezing
- Trigeminal Neuralgia
VIII. Causes: Orthostatic Syncope (Orthostatic Hypotension Syncope, 10% of causes)
- See Orthostatic Hypotension
-
Hypovolemia
- Acute Hemorrhage (Gastrointestinal Bleeding, Ectopic Pregnancy)
- Gastrointestinal losses (Vomiting, Diarrhea)
- Insufficient fluid intake
- Medication-related Syncope (Drug-Induced Syncope, responsible for 5-15% of Syncope causes)
- Recreational drug use
- Postural Tachycardia Syndrome (POTS)
- Most common in female young women (associations with chronic Fatigue and Mitral Valve Prolapse)
- Autonomic failure
IX. Causes: Cardiac Syncope (10-30% of causes, high risk conditions)
- Background
- Results from decreased Cardiac Output from Arrhythmia, structural heart disease or vascular event (e.g. Pulmonary Embolism)
- More likely in known cardiovascular disease (e.g. CAD, CHF, Atrial Fib), first episode after age 35 years
- Associated with no prodrome or prodromal Chest Pain or Shortness of Breath or Cyanosis
- Albassam (2019) JAMA 321(24): 2448-57 [PubMed]
- Predisposing cardiac conditions
-
Arrhythmias
- Ventricular Tachycardia
- Sick Sinus Syndrome
- Supraventricular Tachycardia
- Atrioventricular Block (second or third degree)
- Pacemaker malfunction
- Valvular disorders
- Hypertrophic Cardiomyopathy (esp. young patients)
- Aortic Stenosis
- Acute Mitral Valve Regurgitation (i.e. acute MI with papillary Muscle rupture)
- Prosthetic Heart Valve complication (e.g. Thromboembolism, valvular obstruction)
- Vascular disorders
- Myocardial disorders
X. Causes: Syncope-Plus
- Subset of patients present with Syncope Plus another key symptom
- Acute Painful Syncope
XI. History: Predisposing Conditions
- Family History of Sudden Cardiac Death (e.g. SADS)
- Diabetes Mellitus (Hypoglycemia)
- Parkinson's Disease (Orthostatic Hypotension)
- Seizure Disorder
- Dehydration or blood loss
- Psychiatric illness
- Anxiety Disorder
- Panic Attack
- Hypoventilation
XII. History: Preceeding or provocative event
- Prolonged standing
- Immediately on standing
- While lying supine
- Cardiovascular Syncope (higher risk)
- With exertion (high risk for serious cause)
- See Exertional Syncope
- Aortic Stenosis
- Coronary Artery Disease or Coronary Artery Abnormalities
- Cardiomyopathy (e.g. Hypertrophic Cardiomyopathy, Myocarditis)
- Arrhythmia (e.g. ARVD, Long QT Syndrome, WPW Syndrome, Brugada Syndrome)
- Miscellaneous Causes (e.g. Heat Stroke, Hypoglycemia, Hyponatremia)
- After exertion in an athlete
- Valsalva (cough, Swallowing, eating, laughing, urinating or stooling)
- Reflex-mediated Syncope
- Neck rotation or pressure (e.g. tight collar)
- Use of arms
- Stressful event
XIII. History: Associated symptoms during event
- Nausea, chills and sweats
- Aura
- No prodromal symptoms (see below)
- Cardiovascular Syncope (higher risk)
- Although prodromal Dyspnea or Chest Pain also has been associated with Cardiac Syncope
- Slumping
- Kneeling
- Brief loss of consciousness (<30 to 60 seconds)
- Loss of consciousness (>1 to 5 minutes)
- Seizure Disorder (esp. if postictal period)
- Neurologic, metabolic, or infectious cause
- Tonic-clonic movements
- Seizure Disorder
- Movements occur before fall and last longer than 30 seconds
- Followed by postictal period of confusion
- Syncope (esp. Vasovagal Syncope)
- Movements occur after syncopal fall in 90% of cases
- Appear as Myoclonic Jerks (but brief, <10 movements, and no postictal period)
- Seizure Disorder
- Focal neurologic deficits
- TIA or CVA (although LOC requires significant CNS involvement, for which resolution would be delayed)
- Todd's Paralysis (Seizure)
- Severe Thunderclap Headache
- Chest Pain
-
Palpitations
- Possible Arrhythmia
-
Incontinence of urine or stool
- Seizure Disorder
- Vasovagal Syncope (however, uncommon in Syncope)
- Severe Abdominal Pain or back pain
- Pelvic Pain or Vaginal Bleeding
XIV. Symptoms: Prodromal
- Dizziness
- Vision Loss
- Hearing Loss
- Sensation loss
- Weakness
- Diaphoresis
- Palpitations
XV. Exam
-
Vital Signs
- Temperature
- Blood Pressure
- Orthostatic Blood Pressure (low yield)
- Frequently abnormal in healthy subjects and a majority of the elderly
- However, in elderly, Orthostatic Hypotension may alter disposition and management
- Evaluate patient for symptoms reproduced on standing (more important than measurements)
-
General
- Pallor
- Orthostatic Hypotension due to Anemia
- Tongue bitten
- Ear Exam
- Dix-Hallpike Maneuver
- Pallor
- Cardiovascular examination
- Carotid Bruit (poor Test Sensitivity and Specificity)
- Heart Murmur (evaluate new murmurs associated with Syncope)
- Asymmetric Pulses
- Carotid massage (rarely performed in the acute setting)
- Avoid in Cerebrovascular Disease or Carotid Bruit!
- Used in neurally mediated Syncope to diagnose Carotid Sinus Hypersensitivity
- Congestive Heart Failure findings
- Left-sided Heart Failure (Pulmonary Rales, S3 Gallop Rhythm)
- Right-sided Heart Failure (Jugular Venous Distention, Edema)
-
Abdomen and Pelvis Exam
- Pulsatile mass and decreased Femoral Pulses (Abdominal Aortic Aneurysm)
- Pelvic Pain in a young woman (e.g. Ectopic Pregnancy)
- Rectal Exam (gastrointestinal Hemorrhage)
-
Neurologic Exam
- Post-event Confusion (Seizure Disorder)
- Focal neurologic deficit
- Perform a careful Neurologic Exam to identify subtle deficits
- Red flags suggestive of ongoing active cardiovascular or Syncope-plus cause
- Diaphoresis
- Tachycardia
- Dyspnea
- Significant pain
- Evaluate for injury related to syncopal fall
- See Trauma Evaluation
- Exclude head or neck injury
- Exclude Extremity Injury
XVI. Differential Diagnosis: Serious Causes
-
Arrhythmia
- May be misdiagnosed as Seizure
- Wolff-Parkinson-White Syndrome (WPW Syndrome)
- Brugada Syndrome
- Prolonged QTc >500 ms
- Ventricular Tachycardia
- Structural heart defects and vascular conditions
- Hypertrophic Cardiomyopathy (esp. young patients)
- Aortic Stenosis
- Acute Mitral Valve Regurgitation
- Typically from acute Myocardial Infarction with papillary Muscle rupture
- Prosthetic Heart Valve complication (e.g. Thromboembolism, valvular obstruction)
- Acute catastrophic disorders (Rule of 15s: Each condition has a 15% Incidence as syncopal presentation)
- Aortic Dissection
- Ruptured Abdominal Aortic Aneurysm
- Ruptured Ectopic Pregnancy
- Subarachnoid Hemorrhage
- Acute Coronary Syndrome
- Pulmonary Embolism
XVII. Differential Diagnosis: Non-Traumatic Transient Loss of Consciousness causes
- Seizure Disorder (2%)
- Neurovascular and other neurologic syndromes
- Transient Ischemic Attacks: 1-7%
- Vertebrobasilar Insufficiency
- Subclavian Steal Syndrome
- Dizziness or Vertigo (no loss of consciousness)
- Drop Attacks (No loss of consciousness, no aura)
- Systemic causes
- Muscle Weakness
- Metabolic Disorders
- Mental health disorders
- Acute Intoxication
- Cataplexy
- Psychogenic pseudosyncope
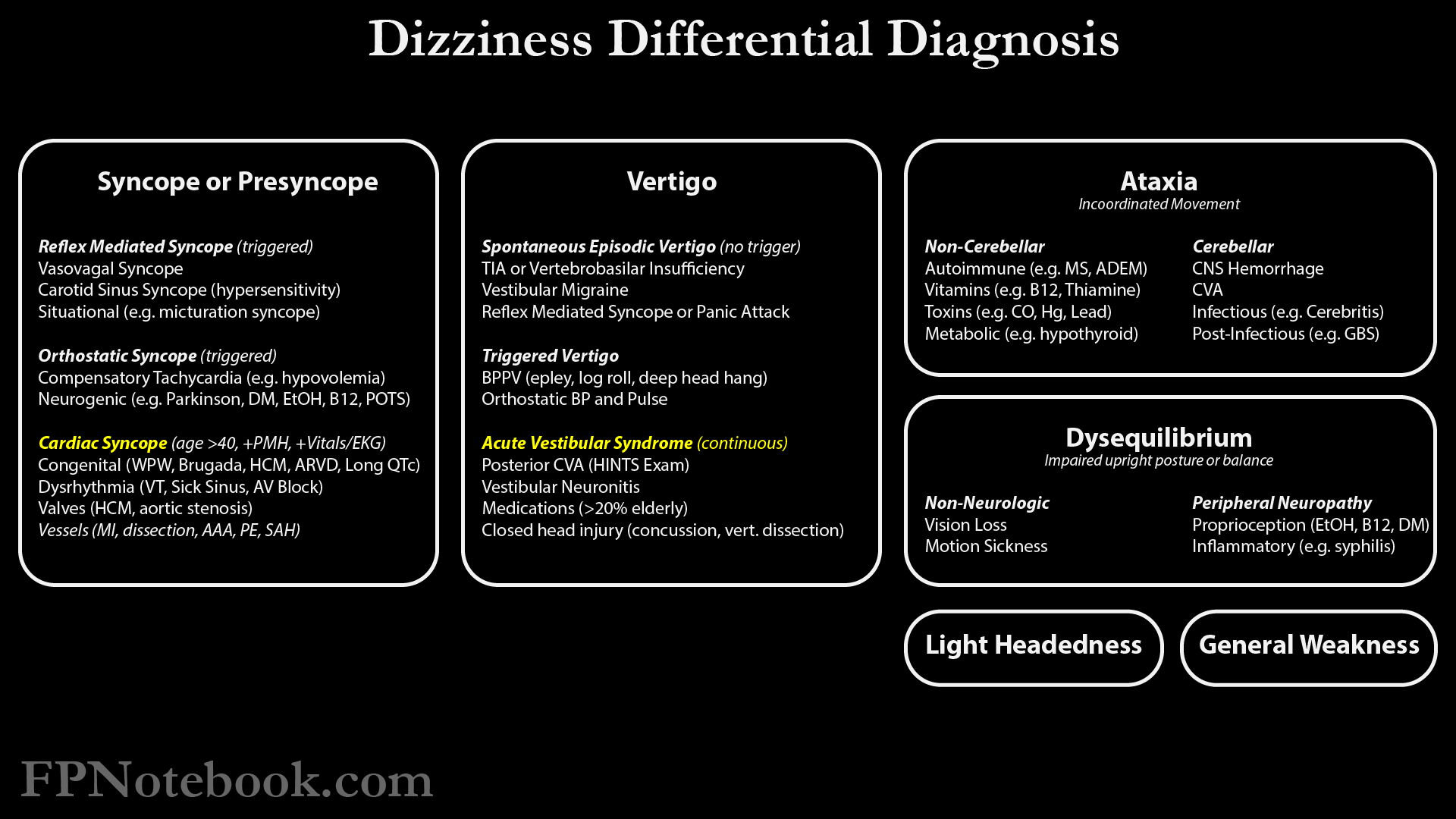
- Images
XVIII. Labs
- Approach
- Targeted blood testing based on history and exam
- Basic Chemistry Panel (Serum Electrolytes including Glucose) Indications
- Low yield in young patients (age <40 years old) without other risk factors
- Bedside Glucose alone may be sufficient in these patients
- Patients warranting chemistry panel
- Patients over age 40 years old
- Prolonged QTc (include Serum Magnesium, Serum Calcium, Serum Potassium)
- Gastrointestinal losses (Vomiting or Diarrhea)
- Diabetes Mellitus
- Chronic Kidney Disease
- Diuretic use
- Dietary restrictions
- Low yield in young patients (age <40 years old) without other risk factors
-
Hemoglobin or Hematocrit Indications
- Blood loss (e.g. Menorrhagia, GI Bleed)
- Comorbidity (HIV, cancer, Renal Failure)
- Signs (pallor, weakness)
-
Pregnancy Test (urine HCG) Indications
- Have low threshold to obtain in women of child bearing age (risk of Ectopic Pregnancy)
- Abdominal Pain
- Vaginal Bleeding
-
Fecal Occult Blood Test Indications
- Anemia
- Associated gastrointestinal symptoms
-
Troponin I
- Associated with a significantly worse outcome if elevated
- However Syncope is a rarely due to ACS or Myocardial Infarction (3% of cases)
- Arrhythmia is a more likely cause of Syncope
- Troponin Is positive in only 1.4% of Syncope patients
- Patients with Syncope due to ACS/MI should still appear ill at evaluation
- Indications
- Chest Pain, Shortness of Breath or other cardiopulmonary symptoms
- EKG with ischemic changes
- References
-
Brain Natriuretic Peptide (BNP)
- Non-specific and unlikely to affect management or disposition
- Earlier studies demonstrated an association with cardiac cause of Syncope
- D Dimer Indications
XIX. Diagnostics
-
Electrocardiogram (EKG)
- See Electrocardiogram in Syncope
- Obtain in all Syncope patients
- However, significant findings in only 5% overall, and 0-3% in those under age 40 years old
- Identify VT, Brugada Syndrome, WPW (short PR), Prolonged QTc >500, Hypertrophic Cardiomyopathy, ischemia
- May assist in distinguishing Seizure and Syncope
- EKG is low yield in syncopal patients under age 40 years old
- Continuous cardiac monitoring (outpatient)
- Indications: Greatest benefit cases
- Cardiovascular disease
- Abnormal baseline EKG
- Syncopal event with associated cardiopulmonary symptoms
- Family History of Sudden Cardiac Death
- Devices
- Holter Monitor (24 to 48 hours of monitoring)
- Consider for daily symptoms
- External Event Monitor (4 to 8 weeks of monitoring)
- Consider for infrequent symptoms (weekly to monthly)
- Patch Monitor such as Zio Monitor (3 to 14 days of continuous monitoring via patch on upper left chest)
- Consider for weekly symptoms
- Implantable loop recorder (may remain implanted for up to 3 years)
- Consider for severe but infrequent symptoms
- Holter Monitor (24 to 48 hours of monitoring)
- Indications: Greatest benefit cases
- Additional tests to consider
- Cardiac stress testing
- Indicated for Exertional Syncope or Angina
- Head-Up Tilt Test
- Indicated for suspected neurally mediated Syncope (distinguishing from Orthostatic Hypotension)
- Hypotension and Bradycardia indicate a positive provocative test
- Cardiac stress testing
XX. Imaging: General
-
Chest XRay
- Low yield test (positive in <0.6% of Syncope patients)
- Abnormal findings (e.g. Mediastinal Widening, Pneumonia, Pneumothorax) are unlikely without physical findings
- Obtain if Chest Pain, Dyspnea, increased Respiratory Rate or Hypoxia
-
Echocardiogram
- Consider in suspected acute valvular cause of Syncope (especially if associated with new murmur)
- Consider if status-post prosthetic Valve Replacement (evaluate for significant valvular dysfunction, obstruction)
- Obtain for EKG consistent with Hypertrophic Cardiomyopathy (High voltage, deep narrow Q Waves)
- Evaluate for Hypertrophic Cardiomyopathy (HOCM), Aortic Stenosis, MI with acute Mitral Regurgitation
- Other imaging to consider
- CT Chest with contrast (if Pulmonary Embolism is suspected)
- Imaging related to injuries sustained in a Syncope-related fall
XXI. Imaging: CT Head
- Efficacy: Low
- Head CT is very low yield in Syncope and not recommended unless indications below
- Goyal (2001) Intern Emerg Med 1(2):148-50 [PubMed]
- Grossman (2007) Intern Emerg Med 2(1):46-9 +PMID:17551685 [PubMed]
- Indications
- Trauma above the clavicles
- Persistent neurologic deficit
- Dizziness
- Sudden onset Headache (Thunderclap Headache of Subarachnoid Hemorrhage)
- Age over 65 years
- Warfarin use
- First Seizure
XXII. Evaluation: Reassuring findings suggestive of non-Cardiac Syncope (low risk Syncope, outpatient evaluation)
- Age <40 to 50 years old
- No cardiac history
- Chronic history of Syncope
- Normal evaluation findings (normal Vital Signs, normal Electrocardiogram, normal Troponin and BNP biomarkers)
- Findings most consistent with non-Cardiac Syncope (neuro-mediated Syncope, Orthostatic Syncope)
- Triggered by specific stimulus
- Noxious smell, sound, sight, pain or other specific trigger (e.g. Cough Syncope, micturation Syncope)
- Prolonged standing, crowded place, heat
- Orthostasis (occurs on standing from supine or seated position)
- Nausea or Vomiting
- Post-meal
- Rotation of head or tight collar, shaving
- Post-exertion
XXIII. Management: Hospitalization or Observation Indications (high risk Syncope)
- Abnormal San Francisco Syncope Rule (CHESS Criteria) or Canadian Syncope Risk Score
- Syncopal episode occurring during Exercise or exertion
- Family History of sudden death
- Severe Orthostatic Hypotension or low systolic Blood Pressure <90 mmHg
- Abnormal Vital Signs
- Severe Anemia (e.g. Hematocrit <30%, gastrointestinal Hemorrhage)
- Significant Electrolyte abnormalities
- Chest Pain or Shortness of Breath with episode
- Sudden onset of Palpitations prior to Syncope
- Advanced age
- Significant underlying cardiac disease
- Congestive Heart Failure
- Severe structural heart disease
- Coronary Artery Disease
- Cardiac Arrhythmia or suspected Arrhythmia
- Abnormal Electrocardiogram
- See Electrocardiogram in Syncope
- Prolonged QTc >500 ms (risk of Torsades de Pointes)
- Type 1 Brugada pattern and new onset Syncope
- Mobitz II AV Block or Third Degree Heart Block
- Persistent significant Bradycardia (Heart Rate <40 bpm not due to fitness)
- Syncope WITHOUT prodrome
- Arrhythmia is more likely if absent prodrome (e.g. Vision dimming, Light Headedness, Nausea, diaphoresis)
- However prodromal Dyspnea or Chest Pain also has been associated with Cardiac Syncope
- References
XXIV. Management: Outpatient
- Approach
- Emergency department discharge is indicated in the absence of high risk criteria (as above)
- Emergency department evaluation identifies 80% of causes
- Additional inpatient telemetry is unlikely to be diagnostic without high risk criteria
- Probst (2019) Ann Emerg Med 74(2): 260-9 [PubMed]
-
Echocardiogram indications
- See imaging above
- Cardiac Event Monitoring (e.g. 7 to 14 day Zio Patch monitor) indications
- Palpitations immediately prior to Syncope
- Prodrome absent prior to Syncope
-
Tilt Table testing (and cardiology Consultation)
- Frequent Vasovagal Syncope episodes
-
Exercise Stress Testing indications
- Not typically indicated in Syncope
- Consider in suspected coronary syndrome related history or findings (typically admit these cases)
XXV. Prognosis
- See San Francisco Syncope Rule (CHESS Criteria) or Canadian Syncope Risk Score
- Predicts short-term risk of serious outcome
- Short-term mortality is relatively low (0.7% at 10 days, 1.6% at 30 days)
- Long-term mortality is however, much higher (8-10% at 6-12 months, esp. Cardiac Syncope)
- Recurrence of Syncope is common (25% in 2 years)
- D'Ascenzo (2013) Int J Cardiol 167(1): 57-62 [PubMed]
- Soteriades (2002) N Engl J Med 347:878-85 [PubMed]
XXVI. References
- Joshi and Dermark (2016) Crit Dec Emerg Med 30(8):3-12
- Orman and Mattu in Herbert (2016) EM:Rap 16(3): 9-11
- Orman and Mattu in Herbert (2018) EM:Rap 18(6): 10-11
- Schauer et al. (2016) Crit Dec Emerg Med 30(9):13-9
- Bayard (2023) Am Fam Physician 108(5): 454-63 [PubMed]
- Brignole (2001) Eur Heart J 22:1256-306 [PubMed]
- Kapoor (2000) N Engl J Med 343:1856-62 [PubMed]
- Miller (2005) Am Fam Physician 72:1492-500 [PubMed]
- Runser (2017) Am Fam Physician 95(3): 303-12 [PubMed]
- Sheldon (2011) Can J Cardiol 27(2): 246-53 [PubMed]