
II. Physiology
- Turbulent Blood Flow results in vibratory changes picked up by stethoscope
- Ventricles fill most rapidly in the first third of diastole
- Aortic Regurgitation murmur is loudest in early diastole
- Mitral Stenosis murmur is also loudest in early diastole (with a slight delay for mitral valve opening)
- Ventricles empty most rapidly in the first third of systole
- However, the Aortic Stenosis murmur is a crescendo decrescendo Systolic Murmur (increases, peaks and decreases)
- Factors that increase murmur intensity
- Increased pressure gradients and velocity changes
- Increased Cardiac Output
- Factors that decrease murmur intensity
III. Images
-
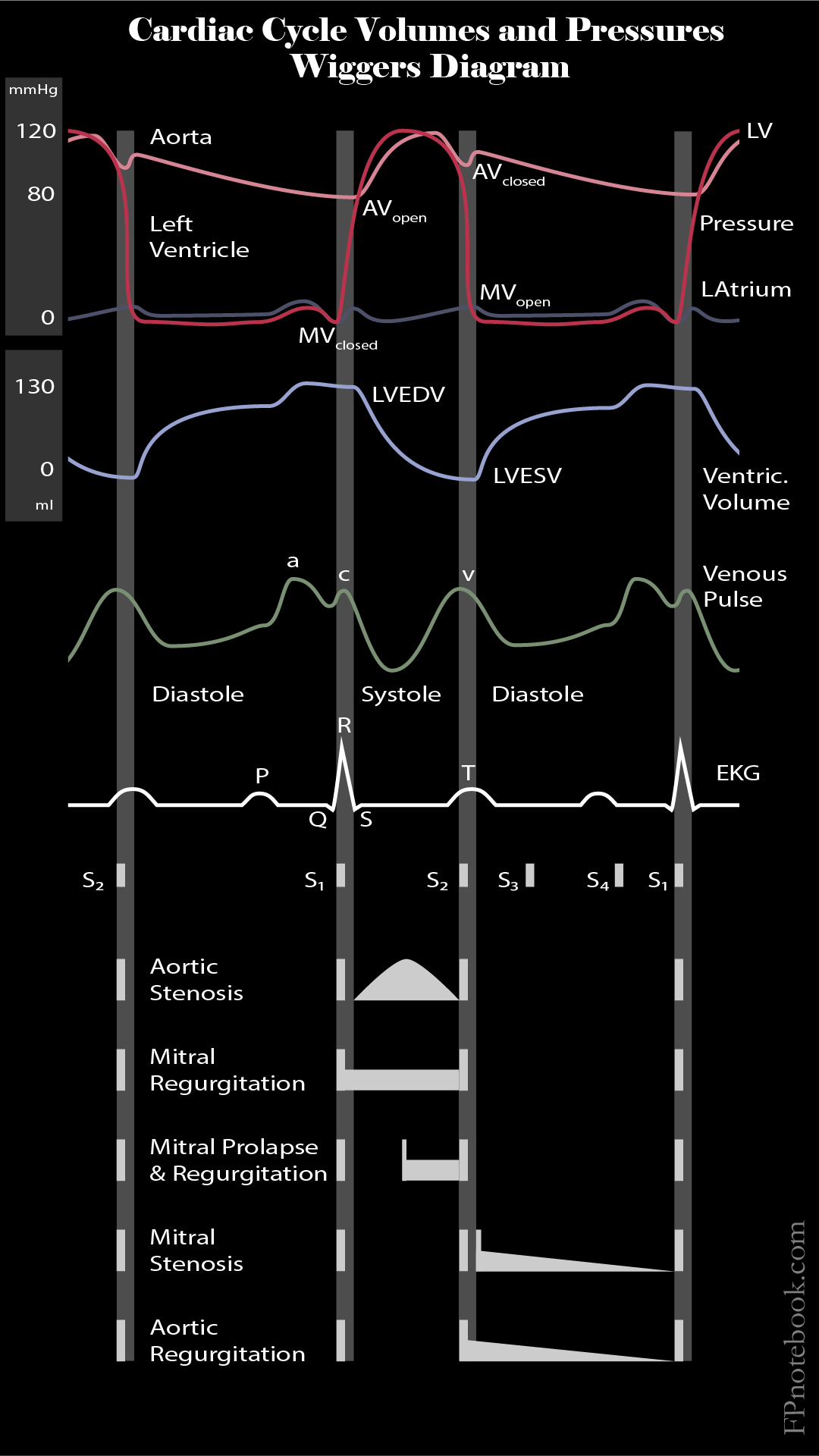
Cardiac Cycle Volumes and Pressures (Wiggers Diagram)
IV. Exam
- Characteristics
- Identify beginning of systole and diastole
- Timing
- Determine timing of murmur
- Systolic Murmur
- Diastolic Murmur
- Continuous Murmur
- Determine Early, Middle or late in interval
- Determine timing of murmur
- Severity
- Grade 1/6: Barely audible
- Grade 2/6: Just easily audible
- Grade 3/6:
- Grade 4/6:
- Grade 5/6: Loudest requiring a stethoscope
- Grade 6/6: Heard with stethoscope off chest
- Location
- Identify valve area involved
- Pattern
- Uniform: Constant
- Crescendo: Increasing
- Decrescendo (Diminuendo): Decreasing
- Crescendo-Decrescendo: Diamond Shaped Murmur
- Pitch
- Low pitched
- Best heard with bell chest-piece at light pressure
- High pitched
- Best heard with diaphragm at firm pressure
- Valve insufficiency murmurs are high pitched due to higher velocity Blood Flow
- Low pitched
- Dynamic Maneuvers: Affecting Left Ventricular Preload (most useful single set of dynamic tests)
- Decreased Left Ventricular Preload (e.g. Valsalva, stand from squat, forced heavy expiration)
- Increases Hypertrophic Cardiomyopathy and Mitral Valve ProlapseSystolic Murmurs
- Decreases Aortic Stenosis, Mitral Regurgitation and innocent Systolic Murmurs
- Increased left Ventricular Preload (e.g. Squat, passive leg raise)
- Increases innocent Systolic Murmurs as well as Mitral Regurgitation and Aortic Stenosis
- Decreases Hypertrophic Cardiomyopathy and Mitral Valve ProlapseSystolic Murmurs
- Decreased Left Ventricular Preload (e.g. Valsalva, stand from squat, forced heavy expiration)
- Dynamic Maneuvers: Other
- Increased Afterload (e.g. hand grip, transient arterial Occlusion with Blood Pressure cuff)
- Increases Mitral Regurgitation, pulmonic stenosis and Ventricular Septal DefectSystolic Murmurs
- Decreases Hypertrophic Cardiomyopathy, Aortic Stenosis and Mitral Valve ProlapseSystolic Murmurs
- Increases Aortic Regurgitation, Ventricular Septal Defect (and possibly Mitral Stenosis) Diastolic Murmurs
- Increased venous return and increased left Ventricular Afterload (e.g. deep or exaggerated inspiration)
- Increases tricuspid regurgitation, pulmonic stenosis Systolic Murmurs
- Increases tricuspid stenosis (and possibly pulmonary regurgitation) Diastolic Murmurs
- Decreased jugular venous return (Jugular Vein compression, or transition supine from sitting)
- Decreases Venous Hum continuous murmur
- Increased Afterload (e.g. hand grip, transient arterial Occlusion with Blood Pressure cuff)
- Consider auscultation in different positions
- Supine
- Erect
- Left lateral decubitus position
V. Interpretation
- Benign murmur findings
- Murmur characteristics
- Crescendo-decrescend character
- Musical or vibratory murmur
- Quiet murmur (Grade 2 or less)
- Timing: Early systolic or mid Systolic Murmur
- Location: Left sternal border or pulmonic area
- Associated findings absent
- Cardiopulmonary symptoms absent
- Family History absent
- Exam (BP, pulse, auscultation) otherwise normal
- Normal physiologic split S2 without gallup or click
- Murmur characteristics
- Pathologic murmur findings
- Murmur characteristics
- Timing: Diastolic, mid-late systolic, holosystolic
- Loud murmur (Grade 3 or greater)
- Murmur exacerbated by Valsalva Maneuver
- Murmur radiates to Carotid Artery or axilla
- Associated findings present
- Arrhythmia present
- Symptoms: Chest Pain, Palpitation, Dyspnea, Syncope
- Sudden Cardiac DeathFamily History
- Jugular Venous Pulsation abnormal
- Arterial pulsation abnormal
- Wide Pulse Pressure
- Water-Hammer Pulse (rapidly rising, bounding)
- Weak, slow rising pulse
- Other abnormal precordial exam
- Other heart sounds (e.g. Loud S1, fixed split S2)
- Left ventricular heave
- Murmur characteristics
VI. Resources
- University of Michigan Heart Sound and Murmur Library