
II. Definitions
- Preload (right atrium Preload)
- Determined by venous return and right ventricular compliance
- End-diastolic wall tension (and end-diastolic volume) of the right ventricle
- Ventricular Muscle stretches in response to increased pressure during diastole
III. Images
-
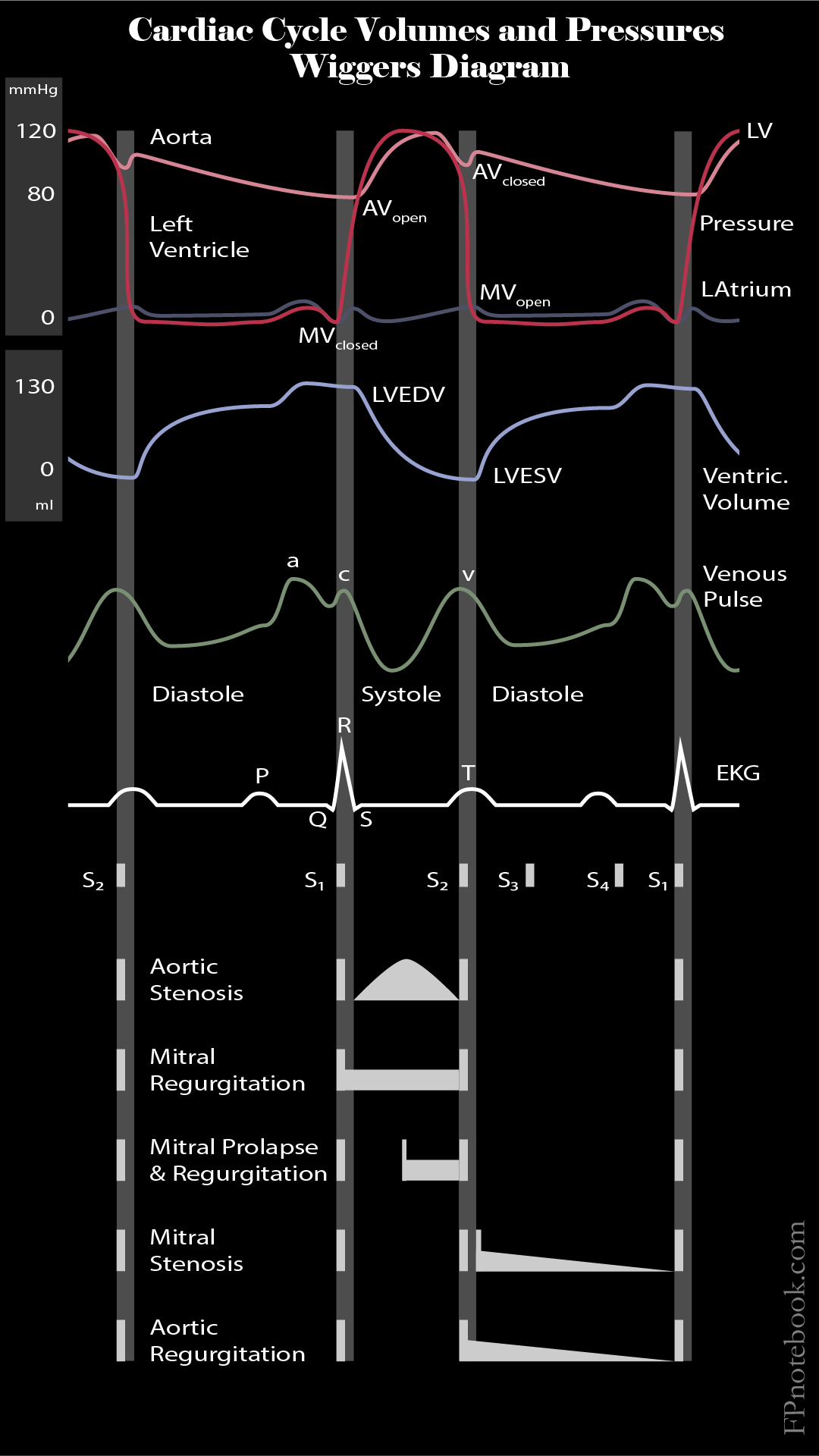
Cardiac Cycle Volumes and Pressures (Wiggers Diagram)
IV. Physiology: Frank-Starling Curve
- Normal heart
- Diastolic volume is the key determinent of ventricular contraction strength in the normal heart
- As end-diastolic volume (and pressure) increases, peak systolic pressure (contraction strength) increases
- Systole starts with isometric contraction (constant Muscle length)
- Contraction against increased ventricular volume with closed aortic valve and pulmonic valve
- Preload is the ventricular wall tension that increases with chamber filling
- Systole transitions into isotonic contraction (constant Muscle tension)
- Systole starts with isometric contraction (constant Muscle length)
- Augmented contractility (e.g. inotrope infusion)
- Frank-Starling Curve shifts up and to the left
- For any given end-diastolic volume, the ventricular contraction (Stroke Volume) is increased
-
Congestive Heart Failure
- Frank-Starling Curve shifts downward and flattens
- For any given end-diastolic volume in CHF
- Ventricular contraction (Stroke Volume) is less than in a normal patient
- Increasing end-diastolic volume in CHF has adverse effects
- Stroke Volume increases minimally (flat part of Frank-Starling Curve)
- Peak systolic pressure increases significantly and results in vascular congestion
- Maladaptive long-term compensatory mechanisms develop to maintain Stroke Volume
- Ventricle dilates (Cardiomyopathy) to allow for increased filling
- Ventricle becomes stiff (Diastolic Dysfunction)
V. Physiology: Effectors of Preload
- Decreased Preload
- Nitroglycerin (vasodilation)
- Diuretics (decreased intravascular volume)
- ACE Inhibitors and Angiotensin Receptor Blockers (vasodilation via suppression of Renin-Angiotensin System)
- Dihydropyridine Calcium Channel Blockers (vasodilation)
- Dehydration
- Increased intrathoracic pressure (e.g. Non-Invasive Positive Pressure Ventilation, Tension Pneumothorax)
- Increased Preload
- Volume Overload (e.g. Congestive Heart Failure, Renal Failure, excessive Intravenous Fluid or transfusion)
- Excessive salt ingestion
- Pregnancy
VI. Diagnostics
- Right Preload
- Central Venous Pressure (see precaution below)
- IVC Ultrasound for Volume Status (Caval Aorta Index)
- Left Preload
- Pulmonary Artery Occlusion pressure or wedge pressure (see precaution below)
- Symptoms (Orthopnea or Dyspnea on exertion)
- Signs (Pulmonary Edema, rales)
- Imaging (Lung Ultrasound)
VII. Precautions
- End diastolic pressure (e.g. CVP and Wedge Pressure) correlates poorly with end diastolic volume even in healthy patients
- Hence CVP and Wedge Pressure are unreliable markers of ventricular filling and volume status
VIII. References
- Killu and Sarani (2016) Fundamental Critical Care Support, p. 93-114
- Marino (2014) ICU Book, 4th Ed Wolters-Kluwer p. 151-7