
II. Indications
- See Advanced Airway
III. Precautions
- See Rapid Sequence Intubation regarding peri-intubation precautions (e.g. Hypotension)
- Intubation attempts should not last >30 seconds
- Limit intubation attempt to 20 seconds in newborns
- Apneic Oxygenation may allow longer safe intubation times
- Optimize first attempt at intubation
- Encourage strategies that increase likelihood of first intubation attempt success (e.g. Video Laryngoscopy, bougie)
- First pass attempt has the lowest complication rate and marked complication rate after 2 intubation attempts
- Mort (2004) Anesth Analg 99(2): 607-13 [PubMed]
- Preoxygenate with 100% Oxygen
- See Endotracheal Intubation Preoxygenation
- Infants and children desaturate very quickly
- Intubation attempts should be brief and stopped as Oxygen Saturation drops below 90%
- Stop and re-oxygenate prior to another attempt
- Consider using an Oral Airway in infants and young children
- Infants have a large Tongue for their small Mandible
- Oral Airway may help keep the Tongue out of the way for the intubation
- Critical to avoid Vomiting during intubation
- Aspiration during intubation can be lethal
- Ensure adequate induction and paralytic dosing
- Rocuronium offers longer paralysis duration and may be considered in difficult airway
- Wait at least 60 seconds following paralytic to minimize Vomiting risk
- Decompress Bowel Obstruction or significantly distended Abdomen prior to intubation
- Consider Nasogastric Tube prior to intubation
- Elevate head of bed
- Avoid aggressive bag-valve-mask technique prior to intubation (prevent Stomach insufflation)
- Exercise extreme caution with awake techniques (careful to avoid gag stimulation)
- Consider pretreatment with Antiemetic
- Two forms of suction on and immediately available
- Open suction tubing
- Yanker suction (or better suction tip such as “S3,” “Big Stick,” and “Big Yank”)
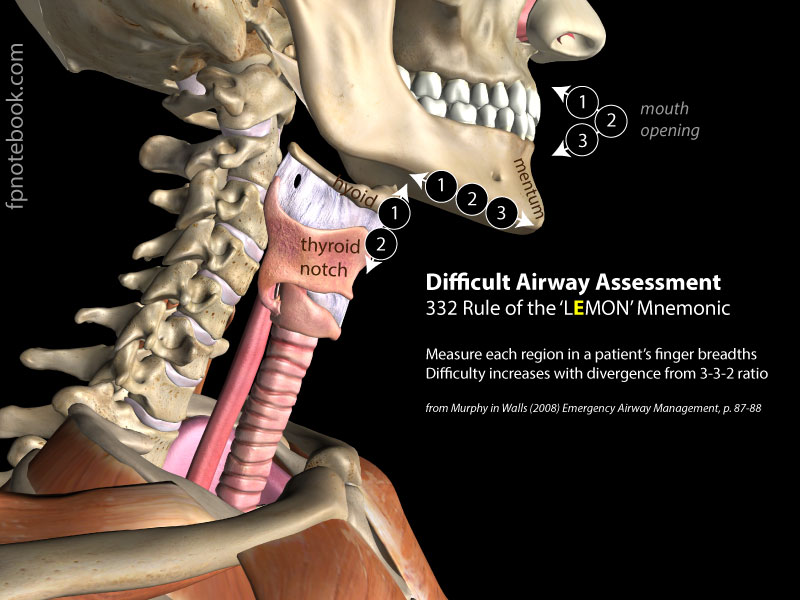
- Anticipate difficult Direct Laryngoscopy (Mnemonic: LEMON)
- Look externally (gestalt)
- Evaluate the 3-3-2 rule
- Significantly more or less than these values suggests more difficult airway management
- Measure each of 3 parameters using patient's own finger breadths
- Three fingers of mouth opening
- Three fingers between mentum and hyoid
- Length >5 cm (adults) is most predictive single factor for first pass success
- Two fingers between hyoid and Thyroid cartilage
- Images
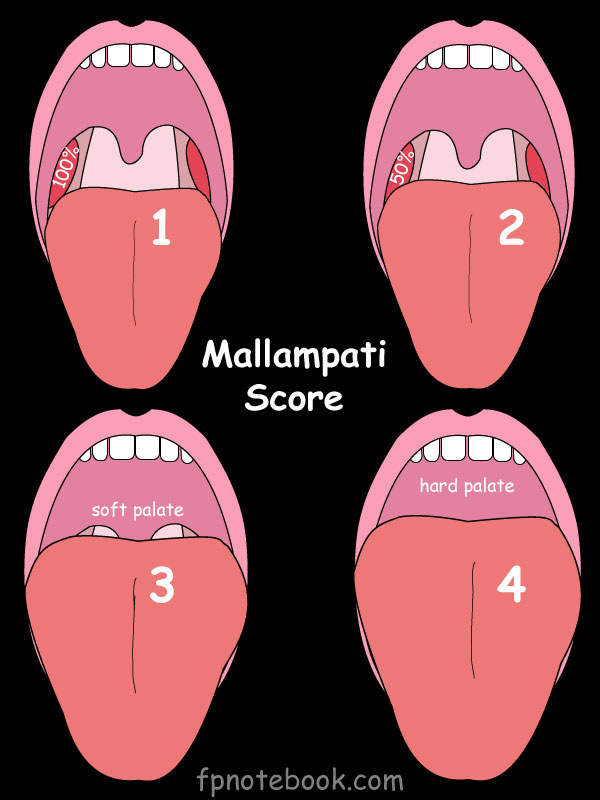
- Mallampati Score
- Class 3 to 4 suggests higher risk
- Class 4 is associated with a 10% failed first pass rate
- Images
- Obstruction ("hot potato voice", inability to swallow secretions, Stridor)
- Severe Angioedema
- Supraglottic swelling
- Smoke Inhalation
- Neck mobility reduced (e.g. Cervical Spine Immobilization, Rheumatoid Arthritis)
- Less of an impact if a hyperangulated blade (e.g. Glidescope) is used
IV. Protocol: Preparation
- See Endotracheal Intubation Preparation
- Includes SOAP-ME Mnemonic
- See Endotracheal Tube (includes Endotracheal Tube Stylet)
- Size and length selection of Endotracheal Tubes
- Lubricate stylet for easy removal (especially with hyperangulated devices such as Glidescope)
- See Extraglottic Device
- Includes Laryngeal Mask Airway or LMA
- Consider as emergency device in case of Endotracheal Intubation failure
- See Endotracheal Intubation Preoxygenation
- Includes Apneic Oxygenation
- Significantly extends duration of safe apnea during intubation
- See Direct Laryngoscope
- Includes sizes of Miller Blade and Macintosh Blade
- See Video Laryngoscope
- Includes Video Laryngoscopy devices such as Glidescope, C-MAC, MacGrath
- Plan and prepare for Post-Intubation Sedation and Analgesia
- See Post-Intubation Sedation and Analgesia
- Verbalize the sedation plan at the time of RSI (sedation should immediately follow ET intubation)
V. Protocol: Positioning
- Optimal head and neck position
- Ear to sternal notch positioning (Levitan)
- Functional Residual Capacity (FRC) is decreased 20% in supine position (as compared with head forward position)
- Head should be forward with ear and Sternum should be at the same horizontal level
- Mandible should also be forward to maximize Thyroid to mental distance (and maximize mouth opening)
- Approximates the tripod position of a child in respiratory distress (head forward and jaw forward)
- Head on pillow(s) flexes the neck forward on the chest and head extended at the neck (Walls)
- Same position as ear to sternal notch position described above
- Sniffing position
- Sniffing position is with the head/neck extended and the face parallel with the ceiling
- Sniffing position is similar to Ear to sternal notch positioning and the Head on pillow position
- Sniffing position is preferred over ramp position, for its better first-pass success, glottic view and less Hypoxia
- Ear to sternal notch positioning (Levitan)
- Children
- Simple maneuvers (e.g. Jaw Thrust) are most effective in children
- Keep head position in midline to prevent soft tissue from obscuring view when head turned to side
- Children age > 2 years (Without C-Spine Injury)
- Head extension with pillow under occiput
- Chin lifted into sniffing position
- Infants age < 2 years
- Large occiput naturally extends the large head
- Chin lifted to sniffing position
- Infants may need a small towel roll under the Shoulders to align the head
-
Trauma
- See Emergency Airway Management
- In-line stabilization technique
- Assistant holds head down on bed, with little fingers applied to each ear to prevent side to side motion
- Remove Cervical Collar completely for intubation
- Load Elastic Bougie in side of mouth
- Orman and Weingart in Majoewsky (2013) EM:Rap 13(4):
- Precautions
- In-line stabilization may be ineffective and potentially harmful
- In-line stabilization significantly prolongs intubation time and decreases first-pass success
- Adjuncts
- See below for techniques to best visualize the cords
- Blood, vomitus or secretions in airway
- See above regarding 2 suctions available, elevated head of bed and aspiration avoidance
- Consider Nasogastric Tube placement prior to intubation
- Be ready with double set-up for failed airway (e.g. Cricothyrotomy with neck marked)
- Consider using suction tip to lead in front of the Laryngoscope (SALAD technique)
- Examiner holds Laryngoscope in left hand and suction in right
- Suction can also be used to retract the right side of the mouth to improve visibility
- May push suction catheter to the left side and leave in place while passing bougie
- Held together with Laryngoscope in left hand
- If catheter tip large enough, may pass suction tip through cords and bougie through catheter
- Bougie will fit through a large bore suction catheter tip (but not a yanker)
- Consider intubation of the Esophagus and inflating the balloon
- Push esophageal ET Tube to the left side (out of the way, but blocking GI secretions)
- Then intubate the trachea
- References
- Strayer in Herbert (2018) EM:Rap 18(11):1-3
- Avoid Cricoid pressure (Sellick Maneuver)
- No longer recommended in 2013
- Worsens airway visualization
- Does not prevent aspiration
- May facilitate glottis viewing if performed correctly (but typically worsens visualization in practical use)
- Optional in 2010 ACC Guidelines
- Does not prevent aspiration
- May impede intubation if performed incorrectly
- No longer recommended in 2013
VI. Technique
- See Rapid Sequence Intubation
- Head and Neck Position are described above
- Hand Position: Infant (reverse for left hand dominant)
- Left Thumb and Index finger hold Laryngoscope
- Left middle and ring finger hold chin
- Left pinky finger pushes down on Larynx
- Right hand inserts ET Tube
- Adjuncts: Elastic Bougie
- Consider holding Elastic Bougie, placed by right molars while positioning Laryngoscope
- Allows for quick placement of Elastic Bougie in difficult airways without losing sight of the cords
- Not helpful in young children due to an incomplete calcification of tracheal rings
- Reference
-
Endotracheal Tube insertion
- Approach: Levitan technique for Direct Laryngoscopy (two landmark)
- Start with "epiglottoscopy"
- Insert Laryngoscope in midline with finger hold at the blade-Laryngoscope junction
- Advance until epiglottis is visualized
- Tongue can be swept at this point
- Visualize arytenoid cartilages (corneiform tubercle, corniculate tubercle) at posterior end of aryepiglottic folds
- Cartilages attach to the vocal ligaments (Vocal Cords) and articulate in and out to open and close the glottis
- Cartilages form a distinct, easily recognizable boundary between Larynx (anterior) and Esophagus (posterior)
- Distinct cartilage appearance alone is an adequate landmark
- Even without direct visualization of the Vocal Cords (upside-down V)
- Visualize the Endotracheal Tube passing anterior to the arytenoid cartilages
- Nearly ensures entry through the Larynx and trachea
- References
- Levitan (2013) Practical Emergency Airway Management Course
- Start with "epiglottoscopy"
- Insert Laryngoscope
- Direct Laryngoscopy
- Levitan recommends inserting in Laryngoscope in midline to visualize epiglottis
- Then sweep the Tongue to side
- Standard technique recommends inserting Laryngoscope into right mouth (at the Tonsillar Pillars)
- Then sweep Tongue to midline
- Levitan recommends inserting in Laryngoscope in midline to visualize epiglottis
- Glidescope (Video Laryngoscopy)
- Insert Glidescope in midline and without Tongue sweep
- Do not insert glidescope too far
- Excessive depth is a very common reason for an inability to pass the ET Tube
- Indications to withdraw Laryngoscope a few centimeters
- ET Tube passage is difficult (also confirm use of hyperangulated stylet)
- Cords are seen at close range
- Direct Laryngoscopy
- Extend blade over base of Tongue
- Insertion location depends on blade type
- Curved blade (Macintosh Blade): Tip into vallecula
- Straight Blade (Miller Blade): Tip over the epiglottis
- Caveat: Curved blades may be used as straight blades (over the epiglottis) and vice versa
- Avoid entering Esophagus first
- Risk of Laryngeal Trauma
- Visualize the epiglottis first and then advance
- Pointers in young children (typically straight blade)
- Insert the blade midline (does not require sweeping Tongue except possibly in syndromic children)
- Avoid inserting the Laryngoscope Blade too far and then pulling back
- Landmarks are difficult to interpret (esopagus may appear similar to trachea in children)
- Insert the blade only to the Tongue base and then lift at a 45 degree angle
- May insert the blade slightly further (millimeter) if the epiglottis still in way
- Insertion location depends on blade type
- Exert traction upward along axis of handle (after epiglottis visualized)
- Straightens the airway for a direct line of intubation
- Do not use teeth or gums as a fulcrum
- Results in significant oral/Dental Trauma
- Exception: Glidescope intubation requires no upward traction
- However airway is not straightened, so must use the glidescope stylet with the deep hockey-stick distal bend
- Due to unstraightened airway with glidescope, unbent ET Tube will be difficult to target the trachea
- Employ techniques to best visualize the cords
- Avoid cricoid pressure (see above)
- Bimanual Intubation Technique (Levitan)
- While left hand holds Laryngoscope, right hand manipulates Thyroid catilage (as in BURP technique)
- Intubating clinician initially manipulates the Thyroid cartilage (instead of assistant)
- Once positioned, assistant may be used to hold position while intubator passes ET Tube
- BURP Alternative in children
- Intubator places their hand over an assistants hand which is in turn held over the anterior neck
- Intubator moves the assistants hand (especially backwards) to align airway
- When cords are well visualized, assistant holds position and inubator removes their hand
- Especially useful in in young children who typically have an anterior positioned Larynx
- BURP Maneuver
- Assistant moves Thyroid cartilage backward, upward and rightward
- Less effective in young children
- Bimanual technique is preferred (see above)
- Tube insertion
- Slow down the Endotracheal Tube insertion (avoid ramming the tube into the airway)
- Avoid obstructing view on tube insertion
- Endotracheal Tube shape in Direct Laryngoscopy should be straight-to-cuff
- Other strategies to avoid obstructing view
- Insert ET Tube from the right corner of mouth
- Hyperangulated devices (e.g. Glidescope)
- See Endotracheal Tube Stylet
- Once tube passes through cords, it will catch on anterior tracheal rings due to hyperangulation
- Stylet must be at least partially withdrawn or tube rotated 90 degrees right (clockwise) to further insert ET
- Hold ET Tube tightly as stylet is pulled out following tube placement
- Stylet may be wedged in tube and can result in dislodging the tube
- Stylet should be pulled out by withdrawing toward the patient's feet (instead of straight up)
- Position ET Tube
- Black marker on ET Tube at level of cords
- Cuffs should be placed just below cords
- See Endotracheal Tube for insertion depths for children
- Typically 23 cm for men, 21 cm for women
- Approach: Levitan technique for Direct Laryngoscopy (two landmark)
VII. Evaluation: Initial Assessment of Tube Position
- Confirming tracheal placement is among the most critically important steps in Endotracheal Intubation
- When in doubt, pull the tube
-
Positive Pressure Ventilations to assess tube position
- Avoid over-ventilating (too fast or with too much volume)
- Hold the bag-valve-mask under-handed like a football hold
- Squeeze with only one hand
- Deliver initials breaths at one breath every 6 seconds in adults
- Observe for symmetric, bilateral chest rise (at a level just below the clavicles)
- Auscultate for equal breath sounds
- Chest auscultation at mid-axillary line (least likely to hear transmitted sounds from epigastrium)
- Assess resistance to manual bag mask ventilation
- Bag compression with properly placed ET Tube should be easy with little resistance
- However, resistance will be increased in poor Lung Compliance and Obstructive Lung Disease (e.g. Asthma)
- After inflating the lungs, air should return rapidly to refill the bag
- Contrast with esophageal intubation associated with resistance to bagging, and poor bag reinflation
- Bag compression with properly placed ET Tube should be easy with little resistance
- Avoid over-ventilating (too fast or with too much volume)
- Other examination findings of proper ET Tube placement
- Document absent breath sounds over Stomach
- Vapor condenses on inside of tube with exhalation
- End-tidal carbon dioxide (End-Tidal CO2 Detector, required by new guidelines 2010)
- May be low if Cardiac Output low (esp. infants)
- Loss of EtCO2 wave form may be loss of pulse (instead of esophageal intubation)
- Check a pulse first, prior to removing an Endotracheal Tube
- Colorimetric EtCO2 may also be used
- Observe color changes (e.g. purple to yellow) after first 5-6 breaths
- Device is purple at CO2 <4 mmHg, partially yellow at CO2 4 to 14 mmHg, and fully yellow at CO2 >14 mmHg
- False Positives have occurred (esp. from gastric insufflation before ET Tube placement)
- False Negatives may occur in Cardiac Arrest and post-ROSC when circulation is too poor to return CO2 to alveoli
- Confirmation with Ultrasound
- Ultrasound can be used to distinguish endotracheal from esophageal intubation
- Place the high frequency probe in Transverse Lie over the anterior midline neck
- Slide the Ultrasound down toward the sternoclavicular notch
- Ultrasound can confirm Endotracheal Tube above carina
- May be performed by a second operator while the other is intubating
- Only one air filled lumen should be present with Endotracheal Tube placement (Esophagus collapsed)
- Two air filled lumens suggests esophageal intubation
- Fill ET Tube balloon with saline and can see the top of balloon at sternal notch
- https://vimeo.com/155465873
VIII. Protocol: Post-intubation Management
- Secure ET Tube
- Confirm tube position again by auscultation
- Note the distance marker at lips in chart
- Commercial tube holder highly recommended
- If holder is not available, tape ET Tube in place and fix to cheek with benzoin
-
Orogastric Tube or Nasogastric Tube (if no Basilar Skull Fracture risks)
- Helps prevent aspiration
- Decompresses Stomach air (gastric insufflation air instilled with Bag Valve Mask)
- Reduces Stomach volume which can interfere with ability to ventilate (especially in children)
-
Chest XRay
- Confirm tube position depth
- Endotracheal Tube should be ~2 cm above the carina and below the level of the clavicles
- Manage Low Blood Pressure (post-intubation Hypotension)
- See Push Dose Pressor
- IV Fluid bolus
-
Post-Intubation Sedation and Analgesia
- See Post-Intubation Sedation and Analgesia
- Adequate sedation is critical to start early (esp. for paralysis with Rocuronium)
- Post-Intubation mechanical Ventilator settings
- See Mechanical Ventilator
- See Ventilator Troubleshooting
- Raise head of bed
- Head of bed to 30 degrees (up to 45 degrees)
- Reduces aspiration risk and improves ventilation
- Decreases Intracranial Pressure in Closed Head Injury
- Avoid raising head of bed >45 degrees (risk of decreased Cerebral Perfusion Pressure)
- Consider bite block
- Protects the Endotracheal Tube from teeth
- Allow for easier orotracheal suctioning
- Consider soft wrist restraints
- Prevents self-Extubation should patient become agitated
- Critical Care
IX. Management: Hypoxemia - Trouble-Shooting Inadequate Ventilation or Oxygenation
- See Ventilator Troubleshooting
- See Mechanical Ventilation
-
DOPE Mnemonic
- Dislodged tube
- Obstructed tube
- Pneumothorax
- Equipment failure
- Detailed approach
- Confirm tube positioned correctly as above
- Is ET Tube too small, cuff under-inflated?
- Is the pop-off valve on Resuscitation bag depressed?
- Higher ventilation pressures are needed with Near-drowning, Pulmonary Edema, and Asthma
- Is the Bag-Valve Device Leaking?
- Compress the bag against an Occluded ET connection (air will be expelled from any leaks)
- Is the operator providing adequate tidal breaths?
- Is there a Pneumothorax present?
- Special Circumstances
- Negative Pressure Pulmonary Edema
- May result from laryngospasm during Endotracheal Intubation or with patient over-breathing Ventilator
- Freezing outdoor Temperatures (e.g. wilderness rescue)
- Endotracheal Tubes may become obstructed from frozen airway secretions
- Shake the tube and suction the material frequently in outdoor cold conditions
- Negative Pressure Pulmonary Edema
X. Management: Post-Intubation Hypotension
- Prevention based on Hypotension Risk Factors
- Pre-Intubation Hypotension, hemodynamic compromise
- Maximize intravascular Resuscitation prior to Endotracheal Intubation if possible
- Optimize with Intravenous Fluids and early Vasopressors prior to Endotracheal Intubation
- Shock Index (heartRate/systolicBP) > 0.8
- Deceptively compensated, normal pre-intubation systolic Blood Pressure
- As with pre-intubation Hypotension, optimize with Intravenous Fluids and early Vasopressors
- Pre-Intubation Hypotension, hemodynamic compromise
- Pre and Post-Intubation Blood Pressure stabilization
- Intravenous Fluid bolus
- Push Dose Pressures (e.g. push dose Epinephrine)
- Evaluate for Endotracheal Intubation Related Causes of Hypotension
- Decreased sympathetic tone (RSI related Anesthetic, esp. Propofol)
- Impaired gas exchange (e.g. esophageal intubation, right mainstem intubation, Pneumothorax)
- Reevaluate tube placement
- Airway Suctioning
- Obtain Chest XRay
- Decreased venous return and Cardiac Output (Positive Pressure Ventilation with increased intrathoracic pressure)
- Higher risk in volume depleted patients
- Obstructive Lung Disease with air trapping and Breath Stacking (large Tidal Volumes, inadequate expiratory time)
- Disconnect the Ventilator to allow exhalation, then manual slow Bag Valve Mask
- Adjust Ventilator settings (decrease Respiratory Rate, permissive hypercapnia, faster inspiratory phase)
- Comorbid conditions
- Cardiogenic Shock
- Right ventricular dysfunction
XI. Management: Post-Intubation Cardiac Arrest
-
Cardiac Arrest occurs in 2-4% of intubated patients
- Occurs twice as often in emergent intubation (in contrast to planned intubation)
- Rhythm is typically Bradycardia or Pulseless Electrical Activity
- Risk Factors
- Advanced age (older patients)
- High Body Mass Index
- Multiple intubation attempts with prolonged apnea
- Hypotension
- Hypoxia
- Severe Metabolic Acidosis
- Reversible Cardiac Arrest Causes
- See Reversible Causes of Cardiopulmonary Arrest (5H5T)
- Evaluate with Bedside Ultrasound (e.g. Pericardial Tamponade, Tension Pneumothorax)
- Peri-Intubation Hypotension (Hypovolemia)
- See Management of Post-Intubation Hypotension above
- Correct with fluid bolus and Vasopressors (e.g. Epinephrine)
- Tension Pneumothorax
- Empirically place bilateral Chest Tubes
- Pericardial Tamponade
- Intubation decreases intrathoracic pressure and Preload
- Esophageal Intubation
- Immediately after ET placement, confirm tube position with Capnography, auscultation
- Use Laryngoscope to recheck ET position and if unclear position, consider Extubation
- Severe Metabolic Acidosis
- Match ventilator Respiratory Rate prior to pre-intubation Respiratory Rate
- Low Respiratory Rates will worsen Metabolic Acidosis (e.g. Salicylate Poisoning, DKA)
- Minimize apnea during intubation
- Optimize chance of first pass success at Endotracheal Intubation
- Sodium Bicarbonate is UNLIKELY to have significant benefit (beyond toxicology use)
- Sodium Bicarbonate relies on Ventilatory effort for expelling CO2
- Sodium Bicarbonate is unlikely to offer benefit over the matched Ventilatory rate
- Match ventilator Respiratory Rate prior to pre-intubation Respiratory Rate
XII. Resources
- Airway Cam (Levitan)
- Airway World (Walls, requires free registration to view videos)
- Glidescope Intubation technique
- Glidescope with 6 intubations
- Elastic Bougie Intubation
- Laryngeal Mask Airway (LMA) Insertion
- CombiTube Insertion
XIII. References
- Copeland and Mehta (2024) Crit Dec Emerg Med 33(9): 27-35
- Dettmer (2021) Crit Dec Emerg Med 35(7): 3-7
- Gausche-Hill and Claudius in Majoewsky (2012) EM-RAP 12(12): 6-7
- Levitan (2013) Practical Airway Management Course, Baltimore
- Majoewsky (2012) EM: RAP-C3 2(5): 3-4
- Roginski, Hogan and Buscher (2020) Crit Dec Emerg Med 34(6): 17-27
- Walls (2012) Emergency Airway Management, 3rd Ed, Lippincott, Philadelphia, p. 63-80