
II. Indications
- Tension Pneumothorax (or suspected Tension Pneumothorax in a decompensating patient)
III. Precautions
- Needle decompression in the second intercostal space, mid-clavicular has significant disadvantages
- Chest wall thickness in obese patients results in a high failure rate
- Needle placement in the second intercostal space is frequently misplaced too low
- Finger Thoracostomy may be preferred over needle decompression
- See Resources below
IV. Equipment
- Child: Size 14 gauge over the needle angiocatheter (5 cm)
- Adult: Size 10 to 14 or 16 gauge over the needle angiocatheter (7.6 cm to 8 cm, 3 inch)
- Needle decompression with 5 cm angiocatheter may fail in 50-60% of adults
- Some studies suggest use of longer needles (8 cm needles are associated with a 90% success rate in some studies)
- Other studies suggest 5 cm catheters should be sufficiently long to reach the pleural space in most adult patients
V. Preparation
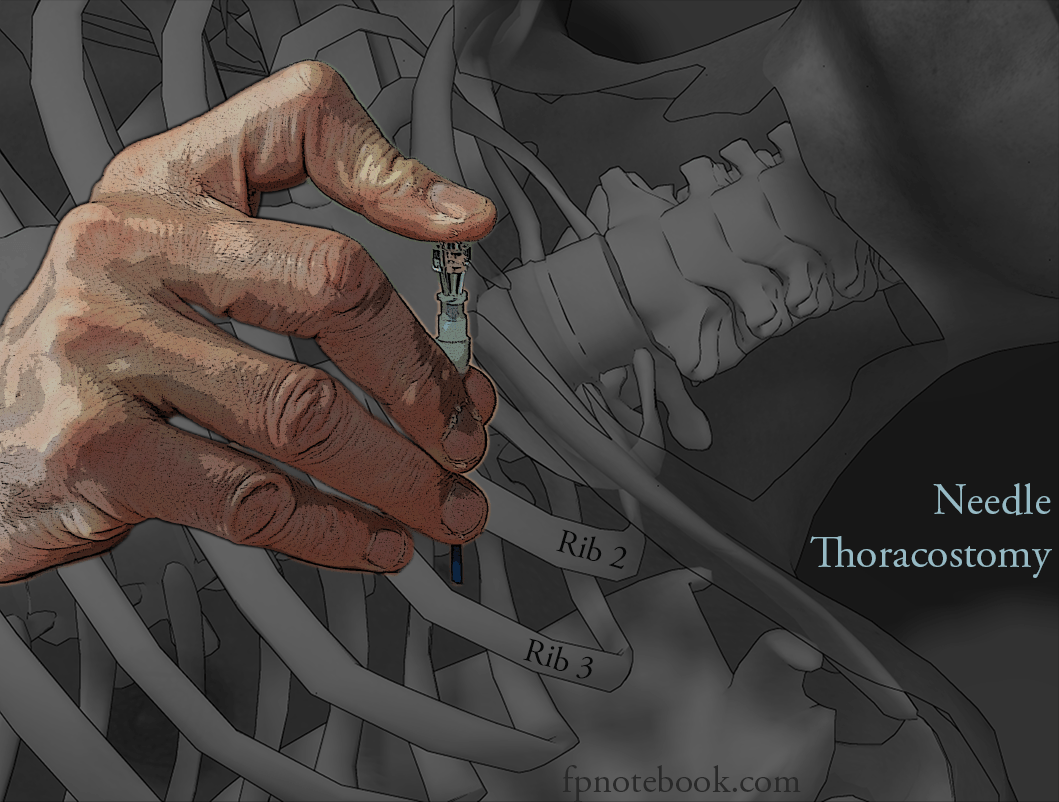
VI. Technique: Needle Thoracostomy
- Images
- Insertion site
- Historical landmark
- Second intercostal space (over 3rd rib) immediately below clavicle (parallel to angle of manubrium)
- Mid-clavicular line (or nipple line)
- Newer proposed landmark
- Anterior axillary line at the 4-5th intercostal space (same as for standard Chest Tube placement)
- Lowest failure rate (shallow chest depth)
- Historical landmark
- Procedure
- Insert angiocatheter immediately OVER the 3rd rib mid-clavicular (or over 5th rib anterior axillary)
- Advance the needle perpendicular (90 degrees) to skin surface
- Signs of needle entering the pleural space
- May feel pop as needle enters pleural cavity
- Rush of air, blood or other chest contents (wear Personal Protection Equipment)
- Vital Signs and clinical status may suddenly improve as Tension Pneumothorax is relieved
- On needle entering chest, hold angiocatheter firmly in place and withdraw needle
- Post-procedure
- Requires Chest Tube placement after initial needle decompression
VII. Technique: Finger Thoracostomy
- Indications
- Traumatic Arrest or Peri-Arrest in evaulation of intrathoracic injury
- Insertion site
- Anterior axillary line at the 4-5th intercostal space (same as for standard Chest Tube placement)
- Procedure
- Perform same procedure as for Chest Tube placement, but instead of inserting Chest Tube, insert finger
- Performed bilaterally
- Post-procedure
- Requires Chest Tube placement after initial needle decompression
- May insert Chest Tube over Elastic Bougie
VIII. Resources
- Regions Trauma Professional's Blog - Needle decompression (Michael McGonigal, MD)
- EM-Crit RACC Needle vs Finger Thoracotomy (Scott Weingart, MD)
IX. References
- Orman and Hicks in Herbert (2018) EM:Rap 18(2): 17-8