
II. Epidemiology
-
Incidence
- In 2013 US: 179,000 bariatric surgeries were performed (42% Gastric Sleeve and 34% Roux-en-Y Bypass)
- In 2017 US: 228,00 bariatric surgeries were performed (60% Gastric Sleeve, 18% Roux-en-Y Bypass)
- In 2019, U.S. 256,000 bariatric surgeries were performed (60% Gastric Sleeve, 18% Roux-en-Y Bypass)
III. Indications: Obesity
- Indications vary depending on organizations (e.g. ACC/AHA, ASMBS, IFSO, AACE/ACE...)
- Body Mass Index (BMI) >= 40 kg/m2 (Class 3 Obesity)
-
Body Mass Index (BMI) >= 35 kg/m2 (Class 2 Obesity) with Obesity-related severe comorbidity
- Primary comorbidity indications
- Type II Diabetes Mellitus or Prediabetes
- Obstructive Sleep Apnea
- Cardiomyopathy
- Nonalcoholic Fatty Liver Disease (NASH)
- Debilitating Lower Extremity Arthritis (e.g. Osteoarthritis of the hip or knee)
- Hypertension
- Hyperlipidemia
- Urinary Stress Incontinence
- Other conditions for which the procedure may be considered
- Obesity Hypoventilation Syndrome
- Idiopathic Intracranial Hypertension
- Refractory Gastroesophageal Reflux disease
- Severe Venous Stasis
- Obesity-related impaired mobility
- Significantly impaired quality of life
- Primary comorbidity indications
-
Body Mass Index (BMI) >= 30 kg/m2 (Class 1 Obesity)
- Diabetes Mellitus with inadequate glycemic control despite optimal lifestyle and medical management
-
Body Mass Index (BMI) >= 27.5 kg/m2
- Asian descent
-
Body Mass Index (BMI) >=25 kg/m2
- Asian descent AND type 2 diabetes or refractory to nonsurgical management
IV. Contraindications
- High risk cardiopulmonary disease
- Ongoing Drug Abuse, Alcohol Abuse or other uncontrolled mental health disorder
- Reversible pathologic causes of Obesity (e.g. endocrine disorder)
- Poor insight into the risks, benefits, lifestyle investment, alternative options, or expected outcomes
V. Mechanism
- Bariatric Surgery results in decreased sense of hunger, increased satiety and increased glycemic control
- Mechanisms go beyond restrictive (small Stomach) and malabsorption (small intestinal bypass) models
- Neuroendocrine responses to Bariatric Surgery play a key role in energy homeostasis
- Glucagon-Like Peptide 1 (GLP-1) increases Insulin secretion
- Peptide YY increases satiety and delays gastric emptying
- Insulin, gherlin, Leptin, c-rp, Interleukin-6, TNF-alpha and adiponectin are all affected by Bariatric Surgery
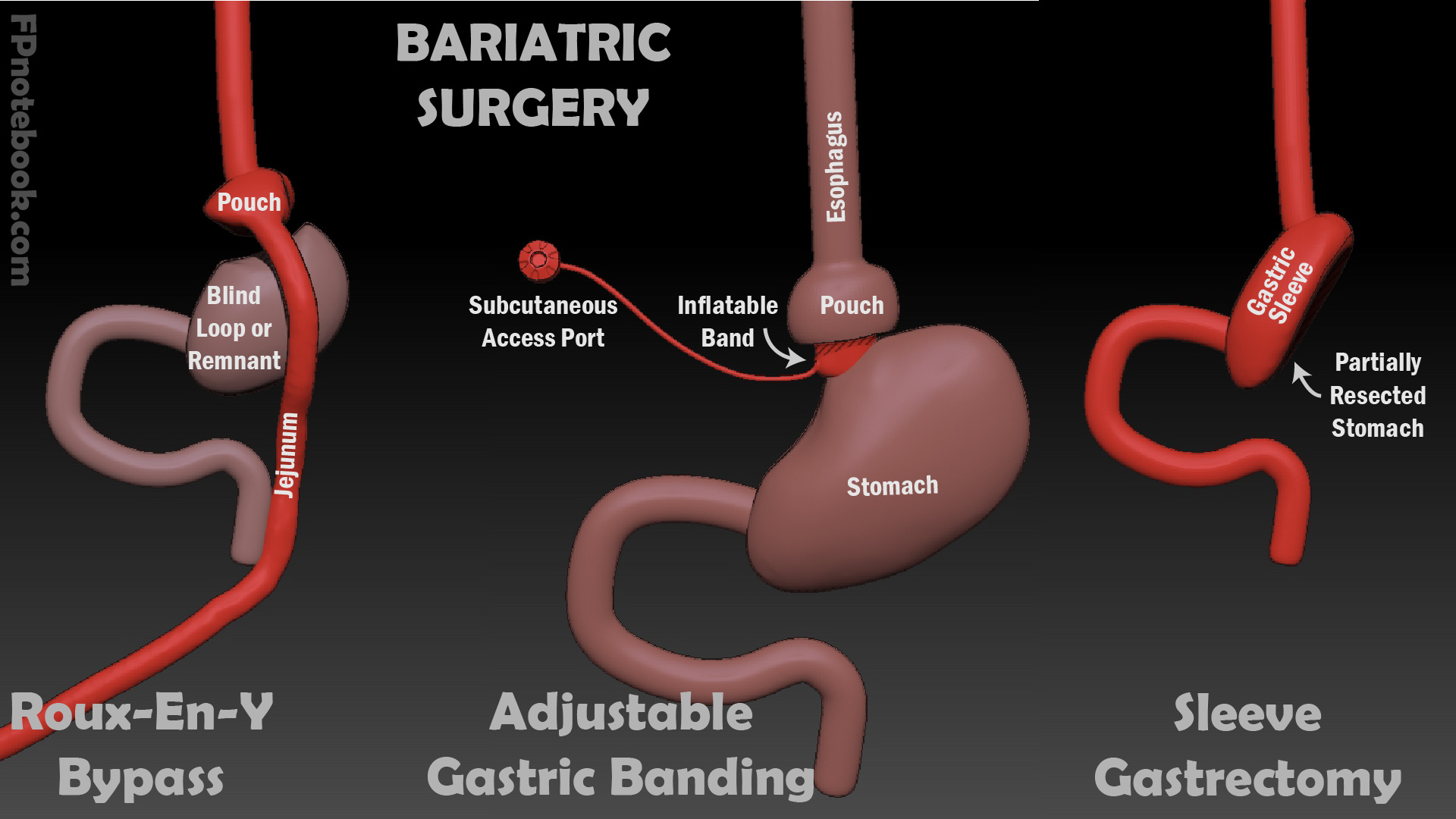
VI. Procedures: Common
- Images
- Roux-en-Y gastric bypass (RYGB)
- Accounted for 34% in 2013 and 18% in 2017 of Bariatric Surgery procedures in U.S.
- Gold standard method today
- Description
- Efficacy
- Weight loss >48% at 1-2 years, >53% at 3-6 years and >25% at 7-10 years
- Diabetes Mellitus remission occurs in 46-81% at 1-3 years
- Safety
- Perioperative mortality: 0.2 to 0.5% within 30 days (0.14 to 0.21% at >30 days)
- Mortality is reduced 30-50% compared to those who did not undergo surgery
- Disadvantages
- Malabsorption of iron, B12 and Calcium
- Technically difficult with higher morbidity
- Gastric Sleeve or Laparoscopic Sleeve Gastrectomy (introduced in 2008)
- Accounted for 42% in 2013 and 60% in 2017 and 2019 of Bariatric Surgery procedures in U.S. (most common)
- Description
- Efficacy
- Weight loss >33% at 1-2 years and >46% at 3-6 years
- Diabetes Mellitus remission occurs in 80% at 1-3 years
- Safety
- Perioperative mortality: 0.296% within 30 days (0.11 to 0.34% at >30 days)
- Mortality is reduced 30-50% compared to those who did not undergo surgery
- Single Anastomosis Duodenal-Ileal Bypass with Sleeve (approved 2020)
- Description
- Combines Gastric Sleeve (as above) with bypass of the duodenum
- Proximal duodenum is anastomosed to the ileum (bypassing the duodenum and biliopancreatic limb)
- Performed at the same time of Gastric Sleeve or as a revision to prior Gastric Sleeve procedure
- Description
-
Laparoscopic Adjustable Gastric Banding (introduced in 2006)
- Accounted for 14% in 2013 and <1% in 2019 of Bariatric Surgery procedures in U.S. (falling out of favor)
- Description
- Efficacy
- Weight loss >29% at 1-2 years, >39% at 3-6 years and >14% at 7-10 years
- Diabetes Mellitus remission occurs in 28% at 1-3 years
- Safety
- Perioperative mortality: 0.02 to 0.07% within 30 days (0.21 to 0.50% at >30 days)
- Surgical Revisions
- Bariatric Surgery revision accounted for 6% in 2013 and 14% in 2017 of Bariatric Surgery procedures in U.S.
- Resources
- Estimate of Bariatric Surgery Numbers 2011-2018 (ASMBS)
VII. Procedures: Other procedures
- Intragastric Balloon
- Balloon inserted via endoscopy
- Reduces Stomach size after inflation
- Left in place for 6 months
- Biliopancreatic Diversion (introduced in 2004)
- Very effective in super-obese patients (BMI>50 kg/m)
- Weight loss 40% at 1 year and 30-40% at 10 years
VIII. Procedures: Not recommended
- These procedures are NOT recommended by NIH panel
- Significantly higher risk of complications
- Jejunoileal Bypass (Distal Gastric Bypass)
- Less commonly performed since 1985 (with a few exceptions)
- Vertical Banded Gastroplasty (VBG or Stomach stapling)
- Less commonly performed since 1989 due to low long-term efficacy
- Replaced by Adjustable Gastric Banding
- Efficacy
- At 3 years: 40-63% excess Weight Reduction
- At 10 years: 20% excess Weight Reduction
- Disadvantages
- Less effective than Roux-en-Y Procedure
- High surgical revision rate (41-45%)
- Due to high rate of staple dehiscence
- Once staple line opens, weight gain returns
- Higher risk of stricture or GERD
- Perioperative mortality: 0-1.0%
- Less commonly performed since 1989 due to low long-term efficacy
IX. Evaluation: Postoperative Complications
- See specific complications below
- Risk Factors for Postoperative Complications
- Preoperative BMI >50 kg/m2
- Age >55 years old
- Male gender
- Pulmonary Hypertension
- Congestive Heart Failure
- Underlying liver disease
- High risk presentations
- Post-operative Fever (red flag)
- Tachycardia (red flag)
- Hypotension
- Tachypnea or Hypoxia
- Bleeding
- Vomiting with Abdominal Pain
- Approach
- Involve bariatric surgeon early in presentation to discuss evaluation and management strategy
- CT Abdomen with oral and IV Contrast (often indicated, but beware False Negatives)
- When performing CT Abdomen, consider CT Chest for Pulmonary Embolism given similar presentations
- Exercise caution with oral Contrast Material due to small proximal pouch
- Avoid harmful measures
- Avoid NSAIDs, Aspirin, Plavix and other irritative agents
- Avoid Nasogastric Tube
- Risk of proximal pouch rupture
- Ineffective at decompression after most bariatric procedures
X. Complications: Acute Serious Complications
- Perioperative Mortality
- Procedure Type
- Roux-en-Y gastric bypass (RYGB): 0.14 to 0.3% mortality
- Sleeve Gastrectomy: 0.08%
- Biliopancreatic Diversion (BPD-DS): <0.3% mortality
- Laparoscopic Adjustable Gastric Banding (LAGB): 0.03% mortality
- Patient factors: Highest risk
- Body Mass Index (BMI) over 60 kg/m2: 3% mortality
- Age over 60 years: 1% mortality
- Patient factors: Additive risks (Mortality increases from 0.2% up to 2.4% if at least 4 criteria are present)
- Age over 45 years old
- Hypertension
- Male gender
- Pulmonary Embolism risk (DVT history, Pulmonary Hypertension, Obesity-related hypoventilation)
- Body Mass Index >50
- Procedure Type
- Thromboembolic complications
- See peri-operative Thromboembolism prophylaxis below
- Pulmonary Embolism is the most common cause of mortality following Bariatric Surgery
- Post-bariatric surgery Pulmonary Embolism is associated with a 20-30% mortality
- Portal Vein Thrombosis
- Gastric Sleeve is the most common surgical cause of Portal Vein Thrombosis
- Presents 7-10 days post-op with diffuse Abdominal Pain, Nausea, Vomiting, Leukocytosis
- Identified on CT Abdomen with contrast
- Emergent consult to Bariatric Surgery and Intervention Radiology
- Initially treated with Heparin (and in some cases catheter directed or systemic Thrombolytics)
- Swaminathan and Shoenberger in Herbert (2020) EM:Rap 20(7):13
- Anastomotic Leak (and secondary Sepsis)
- Leak at anastomosis or banding site
- Roux-en-Y gastric bypass
- Gastrojejunal anastomotic leak (high risk)
- Jejunojejunal anastomotic leak
- Sleeve Gastrectomy
- Staple line leak (high risk)
- Roux-en-Y gastric bypass
- Requires emergency evaluation
- Presentation
- Sepsis signs may initially be subtle
- Severe Abdominal Pain
- Fever
- Hypotensive shock
- Heart Rate over 120 associated with Abdominal Pain increases Specificity
- Tachycardia in first 72 hours after Bariatric Surgery should first be considered an anastomotic leak
- Evaluation
- CT Abdomen with contrast (only 60% sensitive)
- Consider CT Chest for Pulmonary Embolism at the same time (especially if Tachycardia is acute presentation)
- Anastomotic Leak and Pulmonary Embolism may present in similar fashion
- Consider CT Chest for Pulmonary Embolism at the same time (especially if Tachycardia is acute presentation)
- Urgent surgical Consultation
- May require exploration despite negative CT Abdomen
- Early intervention within first 24 hours improves outcomes
- CT Abdomen with contrast (only 60% sensitive)
- Leak at anastomosis or banding site
-
Internal Hernia (occurs in up to 3% of retrocolic bypass procedures)
- See Internal Hernia
- Obtain CT Abomen with contrast
- Requires immediate surgical Consultation
- Bleeding
- Gastric pouch is the most common bleeding source
- Early: Staple Line
- Late: Peptic Ulcer
- Management
- Stabilization as with other Upper Gastrointestinal Bleeding
- Hemodynamic instability may occur earlier due to reduced oral intake after Bariatric Surgery
- Upper endoscopy
- Requires endoscopy operator is skilled at navigating altered anatomy following Bariatric Surgery
- Gastric pouch is the most common bleeding source
XI. Complications: Short-term
-
Small Bowel Obstruction
- Always consider Internal Hernia (see above)
- Avoid Nasogastric Tube (see above)
-
Wound Infection
- Occurs up to 3 weeks after surgery
- Risk of developing Incisional Hernia
- Stomal stenosis
- Presentations
- Early satiety (more than expected)
- Upper Abdominal Pain
- Vomiting even with liquid meals
- Evaluate Upper gastrointestinal series
- Treat with dilatation via upper endoscopy
- Presentations
-
Peptic Ulcer at surgical anastomosis (marginal ulcer)
- Evaluate with upper endoscopy
- Avoid NSAIDs
-
Constipation
- Maximize hydration (96 ounces clear fluid daily)
- Minimize Narcotic Analgesics post-operatively
- Avoid Bulk Laxatives after Gastric banding
- Risk of obstruction
XII. Complications: Long-term
-
Small Bowel Obstruction
- See short-term complications and Internal Hernias above
-
Cholelithiasis or Cholecystitis (30% of patients)
- Consider Cholecystectomy at time of Bariatric Surgery
- Nephrolithiasis related to Calcium Oxalate Stone formation
- Secondary Hyperparathyroidism
-
Gastroesophageal Reflux Disease
- More common with restrictive surgery (Sleeve Gastrectomy, adjustable gastric band)
- Malabsorption (Roux-en-Y Bypass, Duodenal Ileal Bypass with sleeve)
- See lab monitoring below
- See post-operative diet below
- Protein-calorie Malnutrition
- Lipid and Fat malabsorption (decreased enterohepatic circulation)
- Lactose Intolerance
- Beef intolerance (due to heightened Sense of Taste and smell)
-
Vitamin Deficiency (esp. B Vitamins and Fat Soluble Vitamins A, D, E, K)
- Calcium malabsorption
- Micronutrient deficiency
- Copper deficiency
- Zinc Deficiency
- Selenium Deficiency
- Vitamin A Deficiency (night blindness)
- Neuropathy related to Deficiency
- Vitamins B1 deficiency (Thiamine Deficiency)
- Vitamin B12 Deficiency
- Vitamin E deficiency
- Anemia due to Vitamin Deficiency
- Dumping Syndrome (40 to 60% of patients)
- May occur early or late following oral intake
- Early dumping is associated with rapid nutrient flow into the Small Bowel with Fluid Shifts
- Onset within one hour of eating
- Symptoms include Abdominal Pain, Diarrhea, bloating and Nausea
- May also cause Flushing, Palpitations, sweating, Tachycardia, Hypotension, Syncope
- Late dumping is associated with rapid Carbohydrate absorption and exaggerated Insulin response
- Results in Reactive Hypoglycemia onset 1 to 3 hours after eating
- Early dumping is associated with rapid nutrient flow into the Small Bowel with Fluid Shifts
- Management
- Eat small frequent meals
- Avoid rapidly absorbed sugars (e.g. Simple Sugars)
- Avoid fluid with meals
- Consider Acarbose (Precose) to slow CarbohydrateDigestion
- Consider Somatostatin analog
- Surgical revision may be needed in some cases
- References
- May occur early or late following oral intake
- Overall body changes
- Hair thinning (due to rapid weight loss)
- Supplement with more Dietary Protein
- Consider Biotin
- Metrorrhagia
- Fatigue
- Fertility increases
- Use reliable Contraception to avoid pregnancy within first 2 years after surgery
- Food intolerance
- Lactose Intolerance
- Beef intolerance (due to Hypersensitivity to taste and smell)
- Hair thinning (due to rapid weight loss)
- Altered medication absorption
- Gastric banding (gastric restriction)
- Consider switch from XR to immediate release agents
- Take one medication at a time
- Gastric Bypass
- Monitor Digoxin and Levothyroxine dosing closely
- Exercise caution when using Azole Antifungals
- Gastric banding (gastric restriction)
-
Bacterial overgrowth
- Presents with Abdominal Distention, Proctitis, nighttime Diarrhea, and Arthralgias
- Panus (84% of patients)
- Results in local skin irritation, Fungal Infections and discomfort during Exercise
- Paniculectomy indications
- Refractory skin irritation
- Panus severe enough to cover genitalia
XIII. Complications: Lap Band
- Adhesions with Bowel Obstruction
- Port-tubing complications
- Infected port-site with overlying Cellulitis
- Band prolapse
- Presents as A band that is altered from its standard positioning
- Band is normally positioned at a 45 degree angle to the spine
- Band erosion
- Presents as Gastrointestinal Bleeding or Abdominal Pain
- Diagnosis with upper endoscopy
- Band too tight
- May present with pain and Vomiting
- Consider gastrograffin upper GI study or CT Abdomen with contrast
- Consider band deflation (especially if Vomiting and pain)
- Aspirate 4-14 cc fluid from subcutaneous port with a Huber needle
XIV. Efficacy
- Bariatric Surgery is associated with substantial weight loss
- Average of 57 lbs (26 kg) MORE weight loss than non-surgical management
- Total weight loss of 66 to 110 lbs (30 to 50 kg) or 60-70% of excess weight loss (20-30% of total weight)
- BMI decreases 11 to 17 kg/m2
- Gloy (2013) BMJ 347: f5934 [PubMed]
- Bariatric Surgery may cure diabetes in morbid Obesity
- Significantly reduces morbidity and mortality
- Diabetes Mellitus 76% resolved or improved (5 times more likely than in non-surgical management)
- Total and LDL Cholesterol was significantly reduced
- Hypertension resolved in 61% (improved in 78%)
- Sleep Apnea resolved or improved in 83%
- Mortality over 9 years reduced from 28% to 9% (all cause mortality reduction 29-40% across multiple studies)
- Buchwald (2004) JAMA 292:1724-37 [PubMed]
XV. Labs: Monitoring schedule post-procedure
- Three months after surgery
- Six months after surgery
- Nine months after surgery
- One year after surgery and then every year therafter
- Complete Blood Count
- Blood Glucose (or Hemoglobin A1C)
- Serum Creatinine
- Serum Ferritin
- Serum Vitamin B12
- Serum Vitamin D
- Serum Vitamin A
- Other labs to consider
- Serum Thiamine
- Serum Copper
- Serum Zinc
- Serum Magnesium
- Serum Vitamin B6
XVI. Labs: Preoperative evaluation (varies by surgery group protocol)
- Comprehensive metabolic panel (renal and hepatic panel)
- Complete Blood Count with Platelets
- Coagulation studies (INR and PTT)
- Hemoglobin A1C
- Fasting lipid panel
- Thyroid Stimulating Hormone (TSH)
- Vitamin D (25-hydroxyvitamin D)
- Vitamin B12 (Cyanocobalamin)
- Vitamin B9 (Folate)
- Vitamin B6 (Pyridoxine)
- Vitamin B1 (Thiamine)
- Iron Studies (Serum Iron, TIBC, Serum Ferritin)
- Urinalysis
- Urine Pregnancy Test (in all women of child-bearing age with a Uterus)
- Chest XRay
- Electrocardiogram
- Consider RUQ Ultrasound, upper endoscopy, H. pylori testing
XVII. Management: Pre-operative Evaluation
- Preoperative bariatric evaluation is identical to that in non-obese, non-Bariatric Surgery patients
- See Preoperative Exam
- Exceptions: Obstructive Sleep Apnea and Venous Thromboembolism
- Weight loss history and surgery justification is generally completed well before preoperative evaluation
- Encourage Tobacco Cessation to improve healing
- Complete appropriate cancer screening (for age, gender) before surgery
- Evaluation involves a team (primary provider, surgeon, nutritionist, behavioral health)
-
Obstructive Sleep Apnea (not yet evaluated)
- Uncontrolled Sleep Apnea is a significant risk factor for anastomotic leak
- Obstructive Sleep ApneaPrevalence approaches 75% of patients pursuing Bariatric Surgery
- Delay procedure for Sleep Apnea evaluation with formal polysomonography
- If positive for Sleep Apnea, start CPAP and delay surgery for 4 weeks
-
Venous Thromboembolism prophylaxis
- Common (1-3%) and a leading cause of mortality following Bariatric Surgery
- Risk Factors
- Body Mass Index >60 kg/m2
- Chronic Leg Edema
- Obstructive Sleep Apnea
- Prior Thromboembolism
- Estrogens
- Discontinue Estrogen containing Oral Contraceptives 1 month (1 cycle) before surgery
- Discontinue Estrogen containing Hormone Replacement Therapy 1 month before surgery
- Best prophylactic strategy is unclear
- Removable IVC Filters are commonly used in high risk patients (but inadequate evidence)
- Reasonable strategy
- Well-fitted Compression Stockings
- Early ambulation
- Enoxaparin 30 mg bid (40 mg bid if BMI>50)
- Consider removable IVC Filter for high risk patients
XVIII. Management: Post-Operative - General and Diet
- Monitoring of labs (see above)
- Continued education and reevaluation (quarterly in first year, annually thereafter)
- Includes dietician visits, nurse visits and surgical follow-up
- Assess weight, nutritional status, supplementation, symptoms and food intolerance at each visit
- Vitamin Supplementation, as well as nutritional and lab monitoring as above
- Imperative that patients continue life-long care
- Compliance with diet above
- Maintenance of regular physical Exercise program
- Continued behavioral methods to control food impulse
- Consider post-surgical support groups
- Dietary changes to avoid over-distention and Vomiting
- Immediately after Gastric Bypass
- Start with clear liquids and gradually progress to regular foods over first 3 months
- Longterm
- Start meal with Protein portion to ensure adequate Protein intake (80-90 g/day total)
- Cut food into small bite size amounts (as if using toddler utensils)
- Chew well (to applesauce consistency) before Swallowing
- Eat slowly and without distraction (finish a meal within 30 minutes)
- Avoid drinking fluids 30 minutes before and 30-60 minutes after each meal (reduces satiety)
- Avoid carbonated beverages (gas forming)
- Identify fullness Sensation and stop eating immediately when you feel this
- Anticipate and avoid foods likely to be difficult to swallow (dry foods, bread, fibrous vegetables)
- Consider Acute Thiamine Deficiency (Wernicke's Encephalopathy) in acute confusional state presentations
- Empirically dose with 100-500 mg Thiamine IV at presentation
- Immediately after Gastric Bypass
- Other dietary changes
- Limits foods with substantial simple Carbohydrates, Sorbitol or high fats (avoids dumping)
- Stay hydrated by taking 64 ounces non-caffeinated fluid and avoiding Alcohol
- Avoid carbonated beverages
-
Vitamin Supplementation
- Bariatric Multivitamin chewable once to twice daily (twice daily if status-post Roux-en-Y Bypass)
- Vitamin B12 Supplementation (1000 mcg IM monthly or 1000 mcg orally daily)
- Calcium Citrate 1200 to 1500 mg daily (do not take within 2 hours of iron)
- Vitamin D 3000 IU daily (titrate to 25-Hydroxyvitamin D >30 ng/ml)
- Iron Supplementation 45-60 mg/day (may be higher in menstruating women)
- Maintain adequate Dietary Protein intake (see above)
- Additional supplements if deficiency identified (recheck monthly until normal)
- Thiamine 50 mg orally daily for 6 months
- Vitamin B6 50 mg orally daily
- Folate 1 mg orally daily
XIX. Management: Post-Operative - Specific Conditions
-
Type 2 Diabetes Mellitus
- Significant improvement expected after Bariatric Surgery
- Complete Diabetes Mellitus remission in up to 70% following surgery (sustained at 10 years in 38%)
- Insulin requirement eliminated in up to two thirds of patients at 1 year
- Microvascular complications are reduced for up to 20 years after Bariatric Surgery
- Medications
- Avoid agents associated with Hypoglycemia (e.g. Sulfonylureas)
- Decrease Mealtime Insulin (Bolus Insulin) by 50% or eliminate
- Consider decreasing Basal insulin (e.g. Insulin Glargine) by 50 to 75%
- Continue frequent home Blood Glucose Monitoring
- Consider GLP1 Agonist (e.g. Liraglutide) to augment weight loss in first post-operative year
- References
- Significant improvement expected after Bariatric Surgery
- Cardiovascular Disease and Hypertension
- Significant improvement in Cardiovascular Risk Factors after Metabolic Surgery
- Significant reduction in CAD/MI, CHF and new onset Atrial Fibrillation
- Hypertension remission may occur in up to 40% of patients within 5 years of surgery
- However remission is not consistently sustained
- Antihypertensives
- Monitor Blood Pressure including home monitoring
- Blood Pressure decrease may start as early as 2 weeks after surgery
- However Blood Pressure often fluctuates following surgery
- Monitor Blood Pressure in pre and post-operative period
- Do not preemptively stop Antihypertensives (instead, adjust based on monitoring)
- AntiHyperlipidemics (e.g. Statins)
- Monitor and adjust as needed
- References
- Significant improvement in Cardiovascular Risk Factors after Metabolic Surgery
-
Obstructive Sleep Apnea (OSA)
- Nearly 74% of OSA patients were able to stop CPAP at 1 year post-Metabolic Surgery
- Continue CPAP postoperatively
- Obtain Sleep Study after 20% weight loss
-
Osteoporosis (increased risk after Bariatric Surgery)
- Obtain DEXA Scan 2 years after surgery
- Avoid oral Bisphosphonates due to esophageal ulcer risk (at least in short term following Bariatric Surgery)
- Consider IV Reclast or Boniva instead if bisphosphonate needed
- Gallbladder
-
Major Depression and Suicidality
- Major Depression may transiently improve after Bariatric Surgery
- Major Depression has a higher risk of recurrence 12-24 months after Bariatric Surgery
- Inadequate weight loss (or unmet expectations)
- Persistent Obesity related complications
- Weight regain
- Excess, redundant skin after weight loss (e.g. panus)
- Lagerros (2017) Ann Surg 265(2): 235-43 [PubMed]
- Increased risk of Suicidality and self-harm after Bariatric Surgery
- Continue to screen for Major Depression and Suicidality at regular intervals after surgery
- Castaneda (2019) Obes Surg 29(1): 322-33 [PubMed]
-
Alcohol Use Disorder
- Alcohol sensitivity increases significantly after surgery (esp. Roux-en-Y gastric bypass)
- Avoid replacing Overeating with Problem Drinking
- Miscellaneous
- Consider gout prophylaxis
XX. Management: Post-Operative - Women's Health
- Background
- Women represent nearly 80% of Bariatric Surgery patients (and most are of child-bearing age)
-
Contraception
- Ensure reliable pregnancy prevention after Obesity Surgery
- Avoid conception for at least 12-24 months post-op (or stable, with<5% weight loss in last 3-6 months)
- Fetal development may be impaired by rapid maternal weight loss
- Fertility improves as women lose weight (e.g. PCOS improvement)
- Intrauterine Device (IUD) is a preferred effective option in all patients regardless of surgery type
- Roux-en-Y Bypass
- Use non-oral formulations (e.g. Mirena IUD)
- Avoid Oral Contraceptives (decreased efficacy)
- Restrictive procedures (Gastric banding)
- Oral Contraceptives are acceptable option (if not frequently Vomiting)
- However, risk of Venous Thromboembolism (Exercise caution)
- Avoid Ortho Evra patch or drospirenone OCPs due to increased VTE Risk
- Oral Contraceptives are acceptable option (if not frequently Vomiting)
- Pregnancy
- Delay pregnancy for >18-24 months post-procedure (higher risk of adverse outcomes)
- Use reliable Contraception during this time
- Preconception correction of nutritional deficiencies
- Obesity Surgery decreases overall pregnancy-related complication risk
- Lower risk of Preeclampsia
- Lower risk of Gestational Diabetes
- Pregnancy after Bariatric Surgery has different complication risks
- Nutrient deficiency (e.g. Folate Deficiency, Thiamine Deficiency)
- Fetal Growth Restriction and Small for Gestational Age infant
- Supplement
- Protein: Additional extra 10 grams per day
- Vitamin B12: 1000 mcg sublingual weekly
- Folic Acid 800 mg orally daily
- Iron 325 mg orally daily
- Vitamin C 500 mg orally daily
- Calcium 1200 mg orally daily
- Prevent additional weight loss and expect weight gain during pregnancy
- Consider adjustment of Lap band pressure
- Gestational Diabetes screening (at 24-28 weeks)
- Background
- Glucose Challenge Test after Bariatric Surgery is less accurate due to dumping syndrome
- Adustable Gastric banding
- May undergo standard oral Glucose challange test
- Home oral Glucose challange test 1 week protocol
- Background
- Delay pregnancy for >18-24 months post-procedure (higher risk of adverse outcomes)
- Postpartum
- Breastfeeding
- Ensure adequate continuation of Nutritional Supplements
- Postpartum Depression
- Postpartum Depression screening at intervals after delivery
- Breastfeeding
- Gynecologic Cancer Prevention
- Obesity is a risk for Breast Cancer, Ovarian Cancer and Endometrial Cancer (and may be reduced with Obesity Surgery)
- Continue routine cancer screening after surgery
- Lim (2024) JAMA Surg 159(3): 331-8 [PubMed]
XXI. Management: Post-Operative - Medications
-
General formulations and pill size
- Initial first 4 weeks after surgery
- Limit medication forms to liquids, crushable tablets or caplets that can be opened
- Longterm
- Limit medications to plain M&M size or smaller
- Avoid enteric coated or extended release formulation medications (erratic absorption)
- Depending on the surgery, some formulations may be allowed after the first 4 weeks
- Initial first 4 weeks after surgery
-
Analgesics
- Acetaminophen is preferred
- Avoid NSAIDs due to Peptic Ulcer risk and anastomotic ulcers
- Surgeon may approve if absolutely unavoidable, combined with Proton Pump Inhibitor
- Caution with Systemic Corticosteroids
- Medications requiring dose modification (or elimination) as weight loss occurs
- Antihypertensives (see above)
- AntiHyperlipidemics (see above)
- Thyroid medications (e.g. Levothyroxine)
- Diabetes Medications (see above)
- Anticoagulation and antiplatelet agents
-
Venous Thromboembolism prophylaxis
- See Pre-op evaluation above
- May require DVT Prophylaxis for up to 4 months post-op depending on post-op mobility and prior VTE history
- References
- (2013) Presc Lett 20(12): 67-8
- Mechanick (2019) Endocr Pract 25(12): 1346-59 [PubMed]
XXII. References
- (2024) Presc Lett 31(8): 45
- Balsiger (2000) Mayo Clin Proc 75:673-80 [PubMed]
- Banerjee (2022) Am Fam Physician 105(6): 593-601 [PubMed]
- Buchwald (2004) JAMA 292:1724-37 [PubMed]
- Chang (2014) JAMA Surg 149(3): 275-87 [PubMed]
- Choban (1997) J Am Coll Surg 185:593-603 [PubMed]
- Green (2026) Am Fam Physician 113(5): 469-78 [PubMed]
- Virji (2006) Am Fam Physician 73:1403-8 [PubMed]
- Schroeder (2011) Am Fam Physician 84(7): 805-14 [PubMed]
- Schroeder (2016) Am Fam Physician 93(1):31-7 [PubMed]