
II. Definitions
- Atrioventricular Nodal Reentry (AVNRT)
- Form of Paroxysmal Supraventricular Tachycardia (60% of cases) in which reentry occurs within the AV Node
- AV Node in AVNRT contains two pathways (one slow and one fast)
III. Pathophysiology
- Reentry Supraventricular Tachycardia in which the reentry occurs within the AV Node
- Circuit is composed of two pathways, one slow and one fast
- Reentry episode may be triggered by a Premature Atrial Contraction (PAC)
IV. Epidemiology
- Most common overall (60 to 66% of cases) type of Paroxysmal Supraventricular Tachycardia (PSVT)
- Most common in young adults, especially women
- Typically there is no underlying structural heart disease
- Increased onset with low Estrogen and high Progesterone states
- Luteal Phase of Menstrual Cycle (after Ovulation)
- Less common during pregnancy
V. Findings: General
- Heart Rate typically 160 to 190 (up to 260)
- P Waves are often hidden within the QRS (or appear immediately after the QRS)
- Images
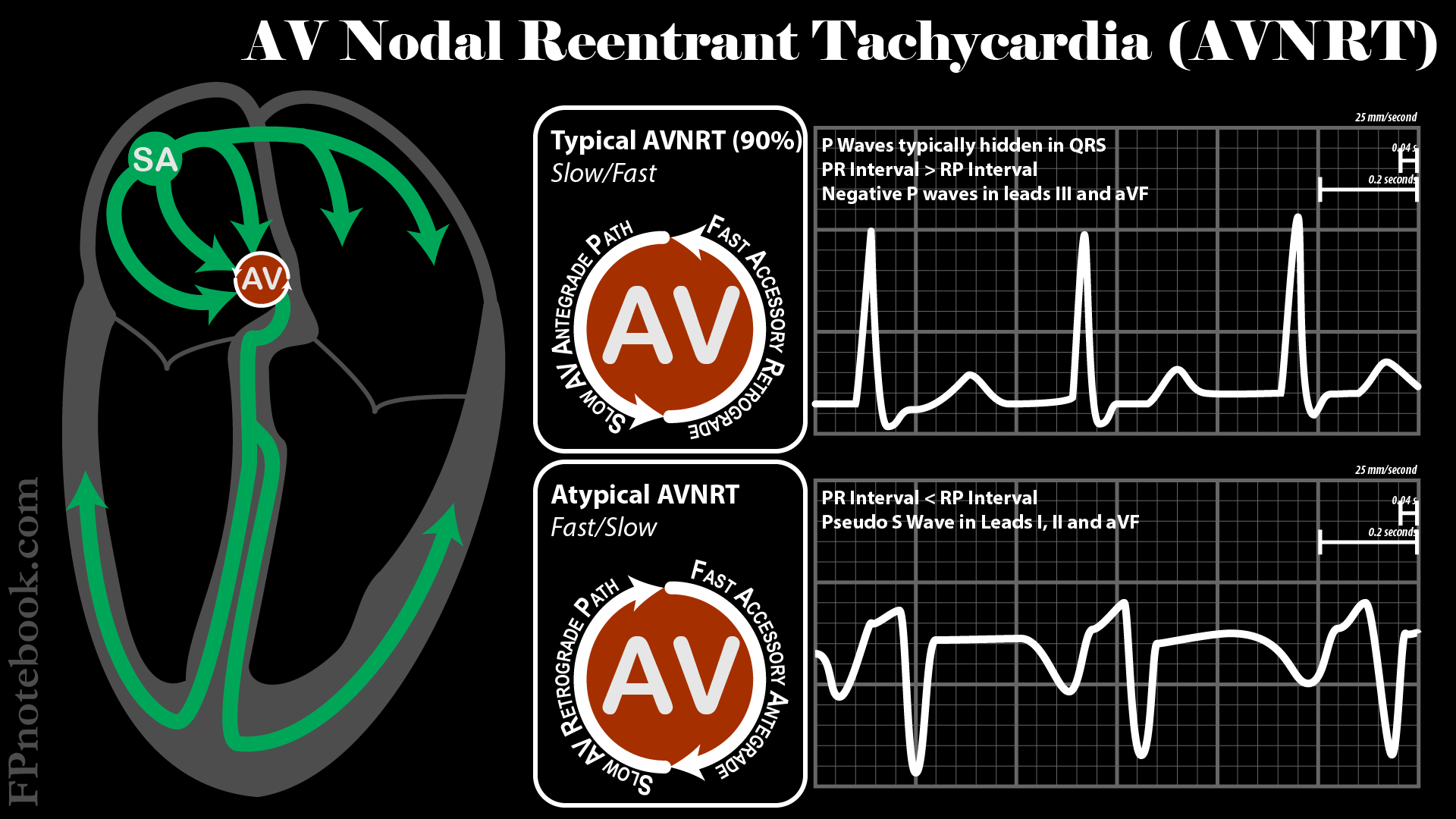
VI. Types: Typical (slow/fast) - 90% of AVNRT
- Course
- Starts with PAC passed down slow accesory path
- Signal travels retrograde up fast path
- Signal cycles back down slow accesory pathway
- EKG findings
- PR Interval > RP Interval
- Negative P Waves in III and avF
VII. Types: Atypical (fast/slow) - 10% of AVNRT
- Course: Reverse of typical pathway
- EKG findings
- PR Interval < RP Interval
- Pseudo-S Wave in leads I, II, aVF
VIII. Symptoms
- Regular, rapid, pounding Sensation in the neck (pathognomonic, LR+ 177)
- Provocative
- Standing up, after bending over
- May occur while lying supine in bed
IX. Signs
- Visible neck pulsations (LR+ 2.7)
X. Management
- Medical Management
- See Paroxysmal Supraventricular Tachycardia
- See Supraventricular Tachycardia
- Patients with Infrequent episodes with tolerable symptoms may wish to continue with only medical management
- Up to 50% of patients will ultimately become asymptomatic and cease to have recurrent PSVT
- Consider longterm suppressive therapy with Metoprolol or Diltiazem
- Catheter Ablation (Electrophysiology)
- First-Line Management for recurrent AVNRT