
II. Physiology: Background
- Images
- Background
- The Menstrual Cycle is a Vital Sign monitor of the hypothalamic-pituitary-ovarian axis
-
Menarche onset in girls (age <11 to 15 years)
- Menses onset after FSH and LH reach sufficient levels
-
Oral Contraceptives (OCP) have a paradoxical effect on the Menstrual Cycle, Ovulation and fertility
- During a normal cycle, FSH triggers a dominant follicle to increase Estrogen, LH surge and Progesterone
- However chronically high Estrogen and Progesterone (e.g. OCP) inihibit Ovulation and fertilization
- Persistent Estrogen inhibits FSH and LH (resulting in no LH surge or Ovulation)
- Persistent Progesterone thickens Cervical Mucus and atrophies the uterine lining
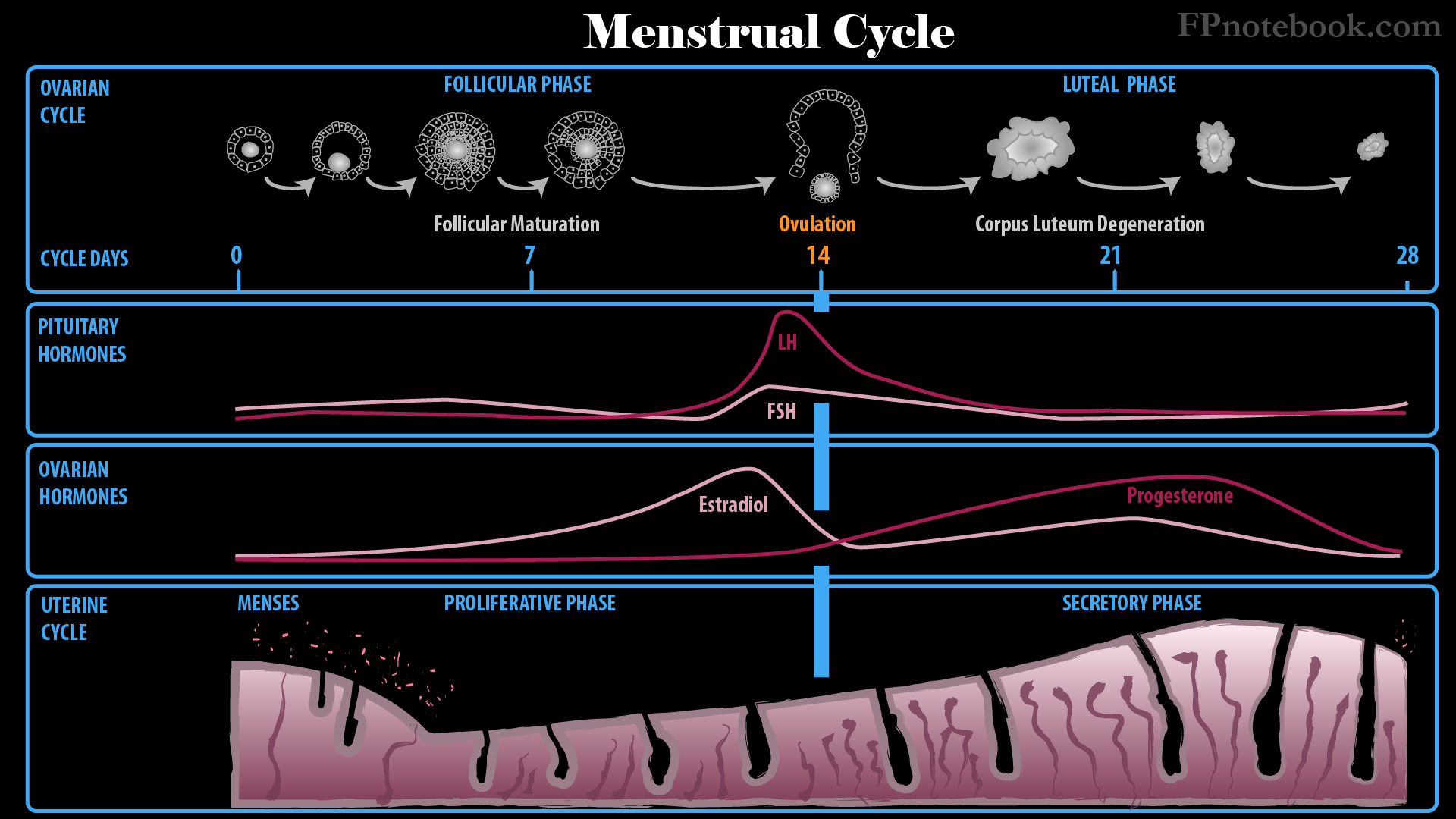
III. Physiology: Follicular Phase (Proliferative Phase in Early Cycle, Days 1 to 13 of cycle)
-
Follicle Stimulating Hormone (FSH) stimulates ovary
- Group of ovarian follicles enlarge, of which one will be dominant, while the other follicles degenerate
- Dominant ovarian follicle emerges days 5-7 of cycle, increasing in size to 2 cm
- Vascularity doubles for dominant follicle
- Twin Gestation prone women generate 2 dominant follicles
- Dominant ovarian follicle produces Estrogen
- Dominant ovarian follicle also contains the ovum which will later be released during Ovulation
- Endometrium proliferative of glands and stroma
- Mean Duration: 10.8 days
-
Hormones low
- Follicle Stimulating Hormone (FSH) low but rising
- Luteinizing Hormone (LH) low but rising
- Progesterone remains low
IV. Physiology: Ovulatory Phase (Mid-Cycle)
-
Hormone Surge
- Follicle Stimulating Hormone (FSH) with small surge
- Dominant ovarian follicle maturation is dependent on FSH stimulation
- Dominant ovarian follicle increases Estrogen release as it matures
- Estrogen rapidly peaks Days 10-15, then decreases
- Estrogen increases with dominant ovarian follicle maturation
- Rising Estrogen triggers a significant increase in LH (and to a lesser extent FSH)
- GnRH is released from Hypothalamus in pulses, in response to rising Estrogen
- GnRH stimulates pituitary LH and FSH release
- Contrast with chronically elevated Estrogen which suppresses LH and FSH release
- LH and FSH may be artificially stimulated in Female Infertility (e.g. Clomiphene)
- Luteinizing Hormone (LH) large surge
- Stimulates Ovulation (2 days after start of surge)
- Typically on day 14 of a 28 day cycle
- Occurs 14 days before Menstruation regardless of cycle length
- Stimulates corpus luteum
- Start of Progesterone increase, with endometrial secretory gland development
- Stimulates Ovulation (2 days after start of surge)
- Follicle Stimulating Hormone (FSH) with small surge
- Mid-cycle Symptoms Include
- Spotting
- Increased vaginal secretions
- Increased libido
- Nausea
- Abdominal Pain (Mittelschmerz)
- Identification of Ovulation Timing
- Fertilization (pregnancy)
- Ovum (egg) fertilized typically within one day of Ovulation
- Sperm (viable for 1 to 3 days after intercourse) typically fertilizes the egg in the fallopian tube
- Fertilized egg exits the fallopian tube into the Uterus within 3-4 days after fertilization
- Ectopic Pregnancy may occur if the fertilized egg fails to reach the Uterus
- Fertilized egg implants within the endometrium 3-5 days after reaching the Uterus
- Implantation occurs 8 to 10 days after Ovulation
- Human Chorionic Gonadotropin (HCG) production starts on endometrial implantation
- See Pregnancy Test (Human Chorionic Gonadotropin)
- HCG (via an LH-like effect) maintains the corpus luteum
- Corpus luteum continues to produce Estrogen and Progesterone
- Estrogen and Progesterone maintain the endometrial lining and prevent sloughing
- Placenta develops from a combination of maternal and Embryonic tissue
- Also produces Estrogen and Progesterone
V. Physiology: Luteal Phase (Secretory phase in Late Cycle)
- Endometrium with secretory gland development (stimulated by Progesterone)
- Prepares uterine endometrium for implantation (should an ovum be fertilized)
- Mean Duration: 13.3 days
- Hormonal changes: Ovum fertilization does not occur
- Estrogen continues to be high days 16-24
- Progesterone surges and remains until days 16-24
- Progesterone depletes Estrogen receptors
- Progesterone level falls to 0 at end of cycle
- Bleeding from Progesterone withdrawal occurs
- Increased Estrogen and Progesterone (as well as Inhibin) decrease FSH and LH via negative feedback
- Luteinizing Hormone (LH) returns to normal
- Follicle Stimulating Hormone (FSH) returns to normal
- Corpus luteum degenerates
VI. Physiology: Menstrual Phase (Bleeding)
- Corpus luteum degenerates
- Estrogen and Progesterone withdrawal
- Sloughing of endometrium with Menstrual Bleeding
- Fibrinolysin secreted by endometrium prevents menstrual blood from clotting
- LH and FSH start to increase again
- LH and FSH are no longer suppressed by Estrogen and Progesterone (via negative feedback)
- Starts a new Menstrual Cycle
- New group of ovarian follicles begins to develop
-
Menopause
- Primordial follicles decrease over time, from Menarche, and eventually resulting in Menopause
- Estrogen and Progesterone production decreases as Menopause approaches
- Normal Menstrual Bleeding per cycle
- See Menses
- Duration: 2-8 days (mean: 4 days)
- Blood Loss: 20-80 ml (mean 35 ml), 13 mg iron loss
- Intervals: 21-35 days (mean 28 days)
VII. References
- Goldberg (2014) Clinical Physiology, Medmasters, Miami, p. 143-5
- Guyton and Hall (2006) Medical Physiology, Elsevier Saunders, p. 1012-5