
II. Epidemiology
-
Prevalence
- General Population: 1.9%
- Emergency Department: 5.5%
- Inpatient: 2.9 to 7.4%
- Brookes (2021) Intern Med J 51(11): 1906-18 [PubMed]
- Kovesdy (2018) Eur Heart J 39(17): 1535-42 [PubMed]
- Singer (2017) Clin Exp Emerg Med 4(2): 73-9 [PubMed]
III. Pathophysiology
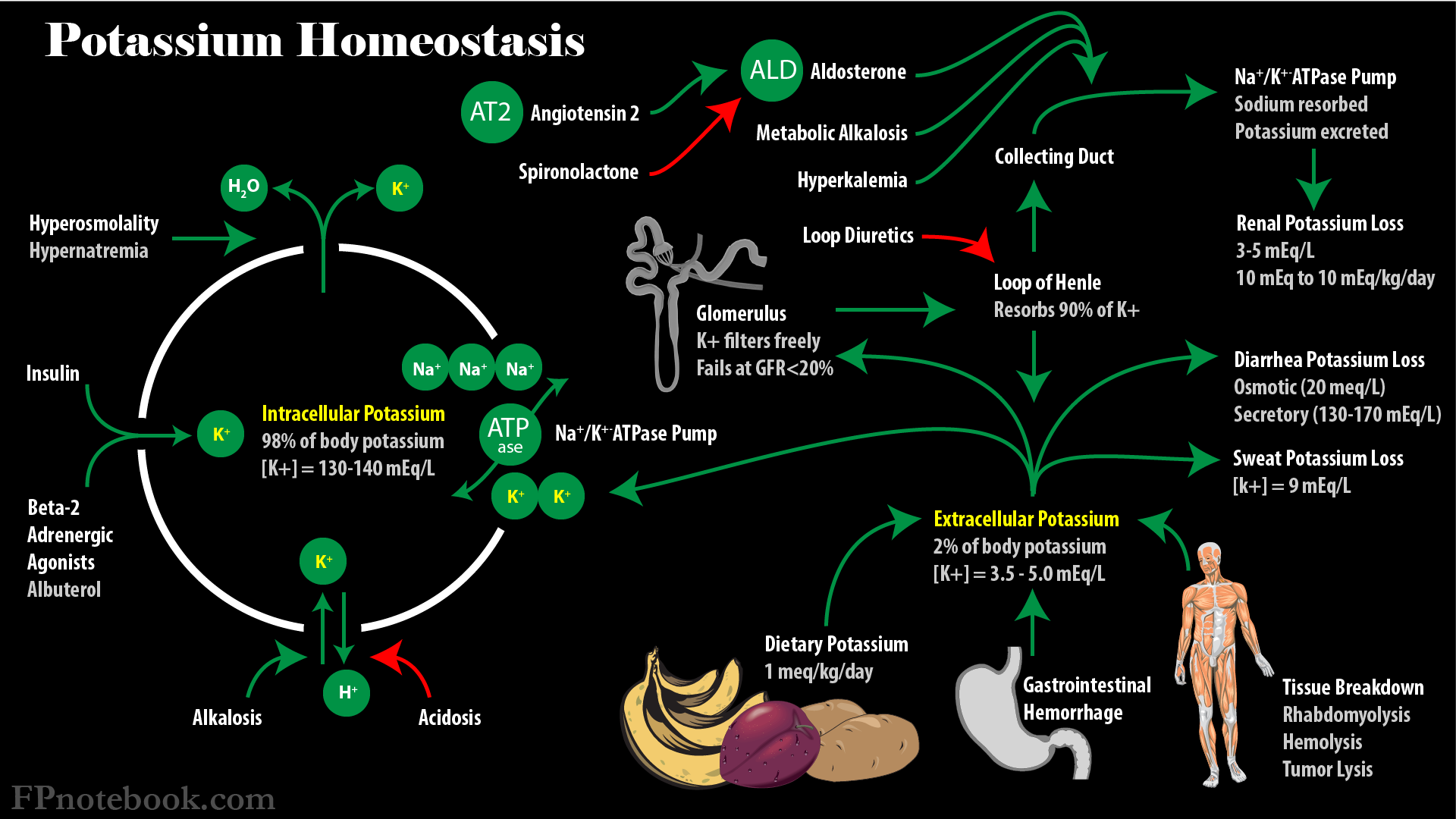
- See Potassium Homeostasis
- See Genetic Syndromes Affecting Serum Potassium and Blood Pressure
- Approximate Total body Potassium = 55 meq/kg
- Serum Potassium decreased 0.3 mEq/L: 100 mEq K+ total body deficit
- Serum Potassium decreased 1 mEq/L: 350 mEq K+ total body deficit
- Serum Potassium less than 2 mEq/L: 1000 mEq K+ total body deficit
- Images
IV. Causes
-
Hypokalemia due to Transcellular Potassium Shift
- See Transcellular Potassium Shift
- Medications (Beta-Agonists, Insulin excess, Caffeine, Theophylline)
- Metabolic Alkalosis
- Hypokalemic Periodic Paralysis
- Thyrotoxicosis
- Hypothermia
- Refeeding Syndrome
-
Hypokalemia due to Renal Potassium Loss
- See Renal Potassium Loss (Hyperkaluria)
-
Hypertension: Obtain Plasma Renin and Aldosterone
- Renin high
- Renovascular disease
- Renin Secreting tumor
- Malignant Hypertension
- Renin normal
- Liddle Syndrome
- Renin low
- Aldosterone High
- Primary Hyperaldosteronism
- Bilateral adrenal hyperplasia
- Aldosterone Low
- Congenital Adrenal Hyperplasia
- Cushing's Syndrome
- Ectopic ACTH
- Exogenous Corticosteroids (e.g. Prednisone)
- Aldosterone High
- Renin high
- Normotensive: Obtain Serum Magnesium, serum bicarbonate and Urine Chloride
- Hypomagnesemia
- Serum Bicarbonate Low
- Renal Tubular Acidosis (Types 1 and 2)
- Serum Bicarbonate High
- Urine Chloride Low: Vomiting
- Urine Chloride High
- Intrinsic renal transport defect (Bartter Syndrome, Gitelman Syndrome)
- Normotensive Primary Hyperaldosteronism
- Diuretic use (Loop Diuretics, Thiazide Diuretics)
-
Hypokalemia due to Extrarenal Potassium Loss
- See Extrarenal Potassium Loss
- Normal Acid-Base Status or Metabolic Alkalosis
- Gastrointestinal or skin losses
- Hypomagnesemia
- Medications (e.g. Penicillin or Aminoglycosides, Sodium Polystyrene Sulfonate)
- Acute Leukemia
- Metabolic Acidosis
- Other causes
- See Drug-Induced Hypokalemia
- Inadequate Potassium intake (typically in hospitalized patients)
- Total Parenteral Nutrition
- Anorexia or Starvation
- Dementia
- Pseudohypokalemia
- Delayed lab analysis of sample
- Severe Leukocytosis (>75,000 to 100,000/mm3)
- Recent Insulin administration
V. Findings: Symptoms and Signs (when Serum Potassium < 2.5 mEq/L or with rapid drop in Serum Potassium)
-
General
- Malaise
- Fatigue
- Neurologic
- Weakness
- Decreased Deep Tendon Reflexes
- Paresthesia
- Cramps
- Restless Legs Syndrome
- Rhabdomyolysis
- Paralysis
- Gastrointestinal
- Constipation
- Ileus
- Exacerbated Hepatic Encephalopathy in Cirrhosis
- Kidney retains Potassium in exchange for Hydrogen Ion, resulting in increased ammonia synthesis
- Cardiovascular
- Orthostatic Hypotension
- Hypertension
- Arrhythmias (rare in otherwise healthy patients)
- Acute or recent Myocardial Infarction (5 fold increased risk of Ventricular Fibrillation if K+ <3.9 mEq/L)
- Digoxin use and Hypokalemia predisposes to Arrhythmia
- Renal
- Metabolic Alkalosis
- Polyuria, Polydipsia
- Decreased GFR
- Glucose Intolerance
VI. Labs
- Serum Potassium <3.5 mEq/L
-
Serum Magnesium
- Confirm no Hypomagnesemia (Hypokalemia cause)
-
Complete Blood Count
- Confirm no severe Leukocytosis (pseudohypokalemia)
- 24 hour Urine Potassium and Urine Sodium
- Most accurate evaluation of Urine Potassium excretion
- However, Urine Potassium-to-Creatinine ratio is typically obtained instead
- Sample should have total Urine Sodium > 100 meq
- Urine Potassium <20-30 meq/day
- Urine Potassium >20-30 meq/day
-
Urine Potassium-to-Creatinine ratio
- Ratio <=1.5 mEq/mmol: Hypokalemia due to Extrarenal Potassium Loss
- Manage underlying losses
- Ratio >1.5 mEq/mmol: Hypokalemia due to Renal Potassium Loss
- Elevated Blood Pressure or hypervolemia (mineralcorticoid excess)
- Metabolic Acidosis
- Type I and II Renal Tubular Acidosis
- Metabolic Alkalosis
- Diuretics
- Renal Tubular transport disorders (e.g. Bartter Syndrome)
- Ratio <=1.5 mEq/mmol: Hypokalemia due to Extrarenal Potassium Loss
VII. Diagnostics: Electrocardiogram
- Early changes
- T Waves decreased amplitude to flattened
- Later changes
- Prominent U Waves
- ST depression (esp. mid-precordial leads, V2, V3)
- T Wave Inversion
- Biphasic T Wave (mid-precordial leads, V1-V3)
- Mattu (2017) Crit Dec Emerg Med 31(3): 11
- PR prolongation (first degree AV Block)
- QTc Prolongation
-
Arrhythmias associated with Hypokalemia
- Sinus Bradycardia
- Ventricular Tachycardia or Ventricular Fibrillation
- Torsade de pointes
- References
- Mattu (2021) Crit Dec Emerg Med 35(3):14
VIII. Management: General
-
Potassium Replacement
- Goal Serum Potassium >3.5 mEq/L (>4.0 in CAD, CHF)
- Expect 0.1 mEq increase in Serum Potassium for every 10 mEq Potassium administered
- Total body Potassium deficit
- Serum Potassium: <3.5 mEq/L = 100 meq total Potassium deficit
- Serum Potassium: 3.2 mEq/L = 200 meq total Potassium deficit
- Serum Potassium: 2.9 mEq/L= 300 meq total Potassium deficit
- Serum Potassium: 2.6 mEq/L = 400 meq total Potassium deficit
- Avoid rebound Hyperkalemia (over-shooting replacement)
- Hyperkalemia with replacement is unlikely if normal Renal Function, adequate fluid intake
-
Dietary Potassium (Potassium phosphate) is less efficient replacement than Potassium chloride
- Most Hypokalemia is associated with concurrent chloride depletion
- However Potassium chloride compliance is poor (Dyspepsia, Dietary Potassium tastes better)
- Half of Potassium Replacement is typically excreted by the Kidneys
- Aside from Renal Failure and Dehydration, at least half of Potassium Replacement (esp. oral) is excreted
- Approximate oral Potassium Replacement
- Start intravenous Potassium Replacement if Serum Potassium <2.5 mEq
- Serum Potassium 2.5 mEq to 3.0 mEq/L (total body deficit 200-300 meq)
- Start with KCl 20 meq orally every 2 hours for 4 doses and consider recheck level at 4 hours
- Typically continue Potassium Replacement at 20 meq twice daily for 4-5 days
- Serum Potassium: 3.0 to 3.5 mEq/L(total body deficit 100-200 meq)
- Give KCl 20 mEq orally every 2 hours for 2 doses OR KCl 40 mEq once
- Typically continue Potassium Replacement at 20 meq twice daily for 2-3 days
- Other Potassium Replacement
- See Potassium Replacement
- Intravenous Potassium Replacement
- See emergent replacement indications below
- Oral replacement other than with Potassium chloride (which is typically preferred)
- Potassium bicarbonate (or oral preparations with citrate or gluconate, or IV Potassium acetate)
- Consider in Metabolic Acidosis with Hypokalemia
- Potassium phosphate (IV)
- Indicated in Hypokalemia with Hypophosphatemia (e.g. Refeeding Syndrome, RTA 2, Fanconi Syndrome)
- Potassium bicarbonate (or oral preparations with citrate or gluconate, or IV Potassium acetate)
-
Magnesium Replacement (empirically or based on lab demonstrated Hypomagnesemia)
- Especially consider empiric Magnesium Replacement in refractory Hypokalemia
- Hypomagnesemia results in Potassium wasting
- Replace Magnesium before Potassium Replacement
- Magnesium Sulfate 2 g IV infusion if Serum Magnesium <1.5 mg/dl
- Magnesium Sulfate 4 g IV infusion if Serum Magnesium <1.0 mg/dl
- Other replacement
- Take oral Magnesium Supplement 400-500 mg tabs 1-2 daily along with Potassium supplement
- Especially consider empiric Magnesium Replacement in refractory Hypokalemia
- Emergent replacement (IV Potassium chloride Replacement) indicated for serious findings or risks
- EKG changes (esp. QTc Prolongation, see above)
- Severe Hypokalemia (Serum Potassium <2.5 mEq/L)
- Rapid onset Hypokalemia
- Serious comorbidity (heart disease, Cirrhosis)
- Cardiac Arrest
- If secondary to Hypokalemia, IV push Potassium chloride 20-40 mEq may be given
- Consider pseudohypokalemia
- Consider re-drawing lab for confirmation if delayed analysis
- Confirm no severe Leukocytosis (WBC >75,000/mm3)
- Consider Transcellular Potassium Shift
- See Transcellular Potassium Shift
- Hypokalemia from transcellular shift is typically transient
IX. Management: Hospital Replacement Criteria
- Hypokalemia with Serum Potassium <3.0 mEq/L AND QTc Prolongation >500 ms
- Severe Hypokalemia with Serum Potassium <2.5 mEq/L
X. Prevention
- Modify Antihypertensive regimen
- Decrease or eliminate Diuretics
- Add ACE Inhibitor or Angiotensin Receptor Blocker (ARB)
- Dietary Changes
- Follow Low salt diet
- Increase Dietary Potassium (may be insufficient to replace Potassium chloride losses)
-
Potassium Supplementation
- Potassium chloride 50 to 75 meq per day increases Serum Potassium 0.14 mEq/L
XI. References
- Orman and Slovis in Herbert (2018) EM:Rap 18(8): 4-5
- Swaminathan and Willis (2025) Hypokalemia, EM:Rap, 6/16/2025
- Kim (2023) Am Fam Physician 107(1): 59-70 [PubMed]
- Viera (2015) Am Fam Physician 92(6): 487-95 [PubMed]