
II. Physiology: Potassium Function
- Cellular Function
- Neuromuscular transmission
- Resting Membrane Potential (large gradient between intracellular and extracellular Potassium concentration)
III. Images
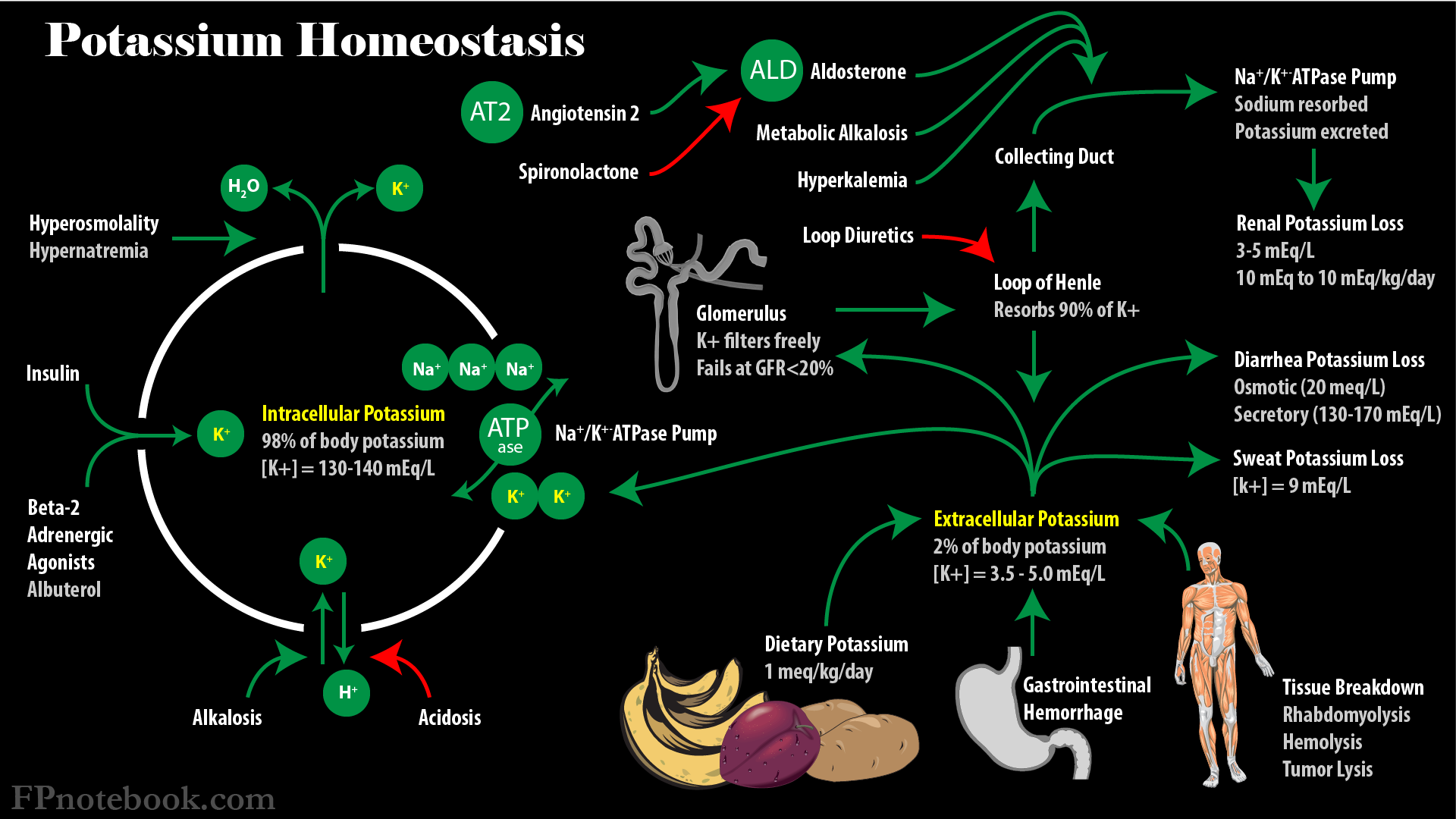
IV. Physiology: Potassium Distribution
- Background
- Potassium is primary intracellular cation and critical for normal cellular function
- Intracellular Potassium concentration of 130-140 mEq/L accounts for 98% of total body Potassium
- Extracellular Potassium (~4 mEq/L) is only 2% of total body Potassium (56 mEq total for entire ECF in 70 kg male)
- Maintenance of intracellular Potassium
-
Transcellular Potassium Shifts
- Mediators that promote Potassium movement INTO cells
- See Hypokalemia due to Transcellular Potassium Shift
- See Hyperkalemia Management
- Insulin
- Alkalosis (Potassium influx exchanged for Hydrogen Ion out of cells)
- Beta 2 Adrenergic Receptor stimulation (e.g. Epinephrine, Albuterol)
- Mediators that promote Potassium movement OUT of cells
- See Hyperkalemia due to Redistribution
- Acidosis (Potassium exchanged for Hydrogen Ion into cells)
- Inorganic acids have a much greater effect on Potassium shifts than organic acids (e.g. lactate)
- Increased Serum Osmolality
- Water flow out of cells concentrates intracellular Potassium
- Potassium gradient favors movement of Potassium out of cells
- Mediators that promote Potassium movement INTO cells
V. Physiology: Potassium Sources
-
Dietary Potassium
- See Dietary Potassium
- Daily intake of 1 mEq/kg typically balances renal (90%) and hepatic (10%) excretion
- Excess Potassium sources
- See Hyperkalemia
- Tissue breakdown
- Rhabdomyolysis
- Hemolysis
- Tumor lysis with Chemotherapy (e.g. Lymphoma)
- Gastrointestinal Hemorrhage
- Potassium is absorbed from the intestinal tract
- Potassium administration
- Blood Transfusion
- Potassium containing medications
- Potassium in Intravenous Fluids
- Tube Feedings with Potassium
VI. Physiology: Renal Potassium Losses (primary excretion)
- See Hypokalemia due to Renal Potassium Loss
- Normal renal Potassium excretion (primary mechanism for Potassium excretion)
- Daily Potassium Excretion range: 10 mEq (in Hypokalemia) to 10 mEq/kg (in Hyperkalemia)
- Relies on intact Glomerular Filtration Rate (GFR), at a minimum >20% of normal
- Potassium at collecting tubule
- Potassium moves freely across the glomerulus, but 90% is reabsorbed in the loop of henle
- Potassium that reaches the collecting tubule (10%) may be adjusted by mechanisms below
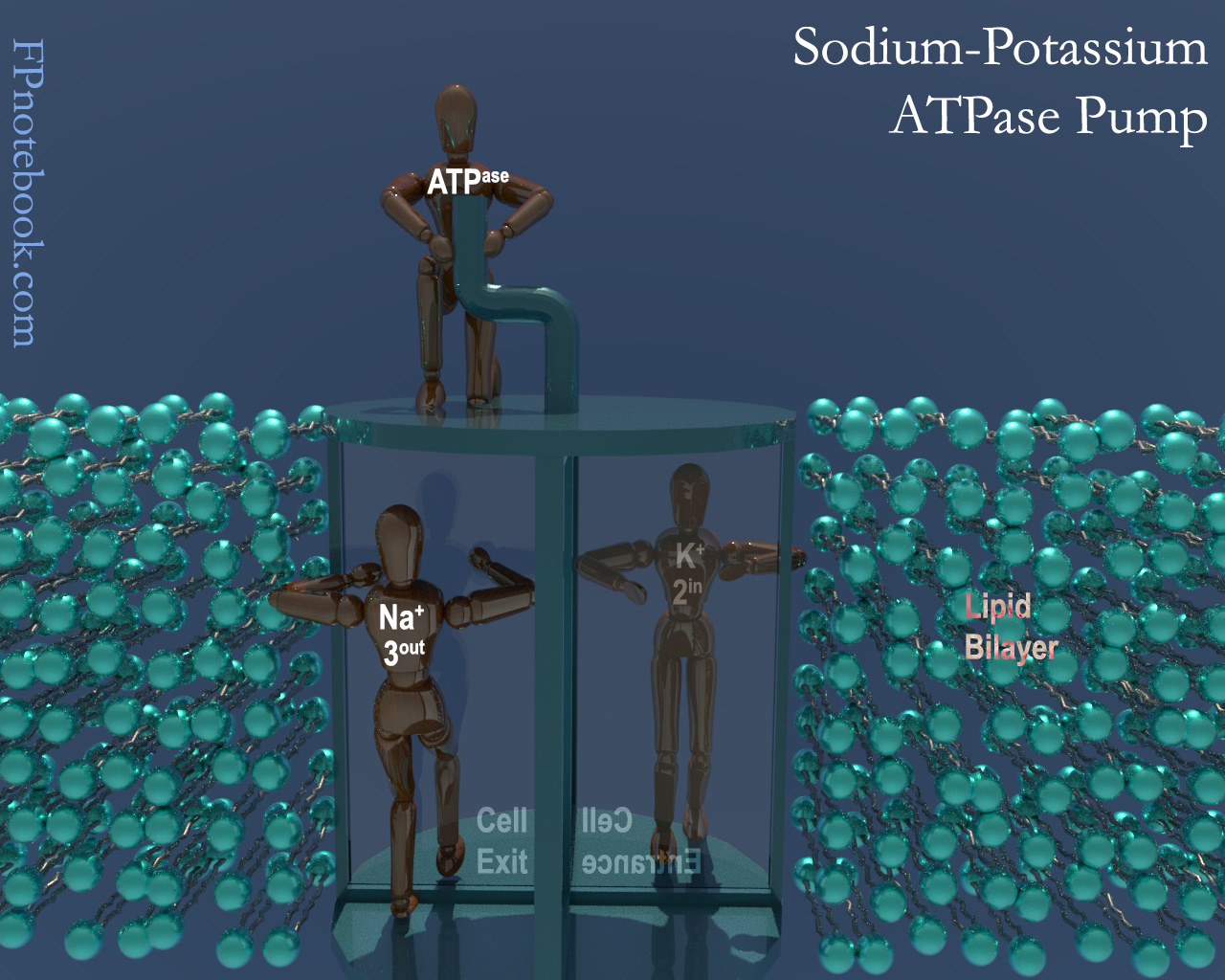
- Potassium excretion by Sodium-Potassium ATPase pump (Sodium exchange)
- Potassium is pumped from the capillary into the cells lining the collecting duct
- Potassium may then flow freely via cell channels into collecting duct lumen toward excretion
- Flows out of the cell's high Potassium concentration
- Flows into the collecting duct lumen, where the Potassium concentration is lower
- Contrast with Sodium which is reabsorbed in exactly opposite fashion
- Factors increasing renal Potassium excretion
- Hyperkalemia
- Aldosterone increase (see below)
- Increased Sodium concentration in the collecting tubule
- Occurs with Diuretics or osmotic diuresis (e.g. Diabetic Ketoacidosis)
- Results in greater Sodium influx into tubule cells with greater ATPase pump activity
- Metabolic Alkalosis
- Bicarbonate is increased anion in the collecting tubule, and is poorly reabsorbed alone
- Bicarbonate is reabsorbed with Sodium, resulting in greater ATPase activity (see above)
-
Aldosterone mediates Potassium excretion (and Sodium reabsorption)
- Aldosterone mediates Sodium-Potassium ATPase pump
- Increasing pump activity results in greater Potassium influx from capillary into the collecting duct cell
- Aldosterone mediates the number of Sodium and Potassium channels on the collecting duct cells
- Increasing the channels allows for greater Potassium outflux into the collecting duct (excretion)
- Factors increasing Aldosterone (and decreasing Serum Potassium)
- Renin-Angiotensin System stimulation (e.g. Hypovolemia)
- Hyperkalemia
- Factors decreasing Aldosterone (and increasing Serum Potassium)
- Aldosterone mediates Sodium-Potassium ATPase pump
- Images: Nephron

VII. Physiology: Extrarenal Potassium Losses
- See Hypokalemia due to Extrarenal Potassium Loss
- Sweat-related Potassium losses
- Sweat contains 9 mEq/L and losses are minimal with typical sweating (200 ml)
- Sweat related Potassium daily loss varies from 2 mEq (normal) to 90 mEq with severe sweating (10 L)
- Gastrointestinal Potassium losses
- Stool losses are typically 10% of Dietary Potassium (7-9 mEq/day)
- Osmotic Diarrhea typically contains 20 mEq/L
- Secretory Diarrhea may contain up to 130-170 mEq/L
- Results in up to >250 mEq Potassium loss daily
- van Dinter (2005) Gastroenterology 129(4):1268-73 +PMID:16230079 [PubMed]
VIII. Pathophysiology: Genetic Syndromes Affecting Serum Potassium and Blood Pressure
-
Hypokalemia with Metabolic Alkalosis and Hypertension
- Renin and Aldosterone suppressed
- Liddle Syndrome
- Congenital Adrenal Hyperplasia
- Apparent Mineralcorticoid excess
- Mineralcorticoid Activating Mutation (Geller Syndrome)
- Renin suppressed and Aldosterone elevated
- Glucocorticoid Remediable Aldosteronism
- Aldosterone producing Adenoma
- Renin and Aldosterone elevated
- Renin and Aldosterone suppressed
-
Hypokalemia with Metabolic Alkalosis and Normal to Low Blood Pressure (and elevated renin and Aldosterone)
- Bartter Syndrome (effects are similar to Loop Diuretics)
- Gitelman Syndrome (effects are similar to Thiazide Diuretics)
- EAST Syndrome (Epilepsy, Ataxia, Sensorineural Deafness, tubulopathy)
-
Hyperkalemia and Metabolic Acidosis
- Renin elevated (and normal to low Blood Pressure)
- Pseudohypoaldosteronism Type 1
- Renin suppressed and Aldosterone normal (and Hypertension)
- Pseudohypoaldosteronism Type 2 (Gordon Syndrome)
- Renin elevated (and normal to low Blood Pressure)
- References
- Baloor (2018) Exam Preparatory Manual for Undergraduates Medicine, Jaypee Brothers, India
IX. References
- Marino (2014) ICU Book, p. 653-72
- Preston (2011) Acid-Base Fluids and Electrolytes, p. 3-30
- Rose (1989) Clinical Physiology of Acid-Base and Electrolyte Disorders, p. 3-27