
II. Images
- AcidBaseNomogram
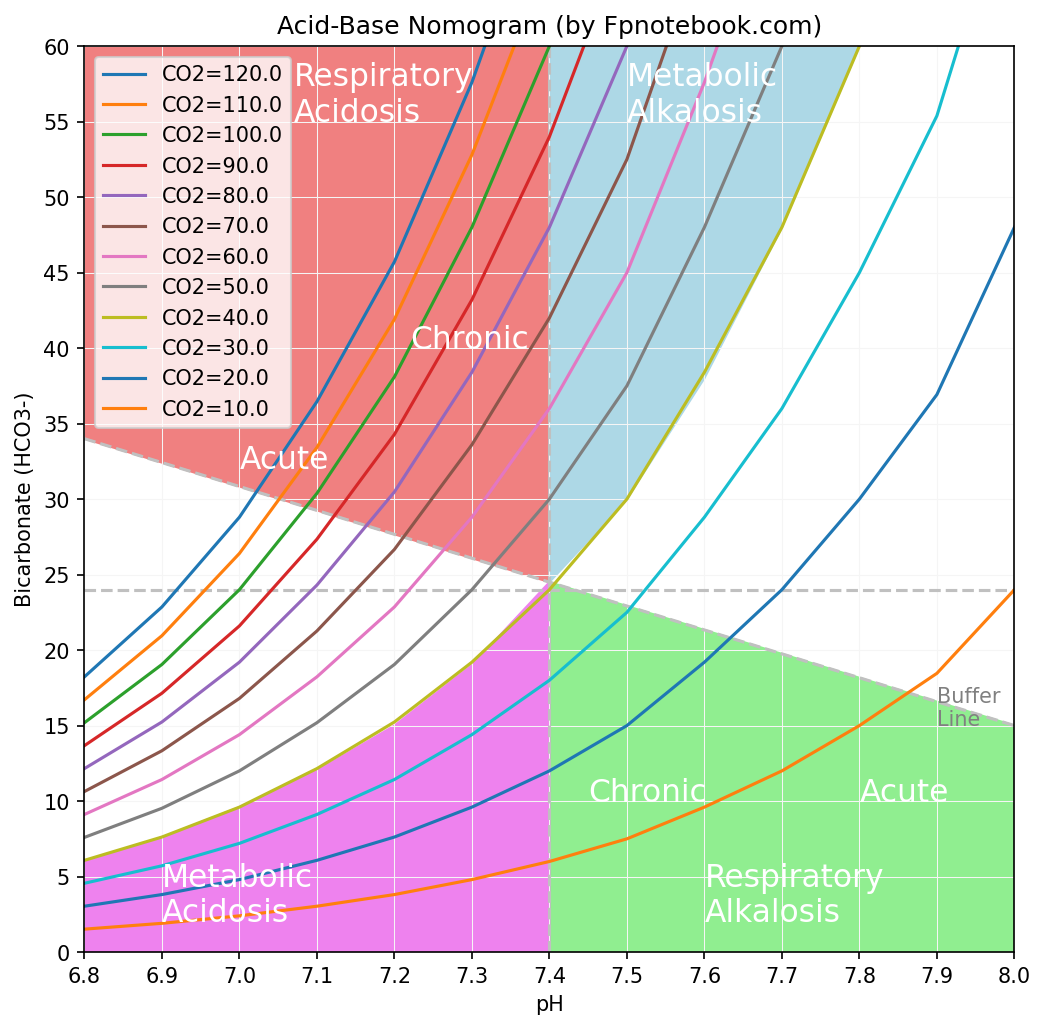
III. Technique: Step 1 - Determine primary abnormality
- Determine Acidosis versus alkalosis
- pH >7.45: Alkalosis
- pH <7.35: Acidosis
- Determine Metabolic versus Respiratory
- Primary Metabolic Disorder
- pH changes in same direction as bicarbonate, pCO2
- Metabolic Acidosis (increased acid other than CO2 or bicarbonate loss)
- Serum ph decreased
- Serum bicarbonate decreased
- pCO2 decreased (when compensated with increased Respiratory Rate)
- Metabolic Alkalosis (e.g. protracted Vomiting with gastric acid loss)
- Serum ph increased
- Serum bicarbonate increased
- pCO2 increased (when compensated)
- Primary Respiratory Disorder
- pH changes in opposite direction bicarbonate, pCO2
- Respiratory Acidosis (e.g. apnea or Respiratory Failure)
- Serum ph decreased
- pCO2 increased
- Serum bicarbonate increased (when compensated)
- Respiratory Alkalosis (e.g. Hyperventilation)
- Serum ph increased
- pCO2 decreased
- Serum bicarbonate decreased (when compensated)
- Mixed Disorders
- Serum Bicarbonate and pCO2 are altered in opposite directions
- Mixed Respiratory Acidosis and Metabolic Acidosis
- Serum pH decreased
- pCO2 increased
- Serum bicarbonate decreased
- Mixed Respiratory Alkalosis and Metabolic Alkalosis
- Serum pH increased
- pCO2 decreased
- Serum bicarbonate increased
- Primary Metabolic Disorder
IV. Technique: Step 2 - Sharpen the diagnosis
- Calculate the Anion Gap
- Useful in Metabolic Acidosis
- Useful in mixed acid-base disorders
- Anion Gap = sNa - sCl - sHCO3
- Where sNa = Serum Sodium, sCl=Serum Chloride, sHCO3=Serum Bicarbonate
- Normal Anion Gap = 8-12 meq/L
- Anion Gap is maintained by near balance of key cations (sNa+) and key anions (sCl-, sHCO3-)
- In Non-Anion Gap Metabolic Acidosis, only measured cations and anions are affected
- In Diarrhea, bicarbonate is lost and compensated by chloride increase
- In Anion Gap Metabolic Acidosis, unmeasured anions are increased
- Increased Lactic Acid or Ketoacids, for example, result in a significant Anion Gap
- In Non-Anion Gap Metabolic Acidosis, only measured cations and anions are affected
-
Excess Anion Gap (EAG)
- EAG = Anion Gap - 12 meq/L + serum bicarbonate
- Interpretation
- EAG > 30 mEq/L: Metabolic Alkalosis present
- EAG < 23 mEq/L: Non-Anion Gap Metabolic Acidosis
- Gap-Gap Analysis
- Calculate Osmolar Gap
- Useful in Metabolic Acidosis with Anion Gap
- Calculate Urinary Anion Gap
- Useful in Non-Anion Gap Metabolic Acidosis
- Distinguishes renal from extra-renal cause
V. Technique: Step 3 - Determine Compensation
- Metabolic Acidosis
-
Metabolic Alkalosis
- PaCO2 increases 6 mmHg per 10 meq/L bicarbonate rise
- Acute Respiratory Acidosis
- Chronic Respiratory Acidosis
- Metabolic compensation after a few days of Respiratory Acidosis
- pH decreases 0.03 for each 10 mmHg PaCO2 increase from 40 mmHg
- Bicarbonate increases 3.5 to 4 meq/L per 10 mmHg PaCO2 rise from 40 mmHg
- Acute Respiratory Alkalosis
- Chronic Respiratory Alkalosis
- Metabolic compensation after a few days of Respiratory Alkalosis
- pH increases 0.03 for each 10 mmHg PaCO2 decrease from 40 mmHg
- Bicarbonate decreases 5 meq/L per 10 mmHg PaCO2 decrease from 40 mmHg
- Minimum bicarbonate in respiratory compensation is typically 12-15 meq/L
VI. Technique: Step 4 - Define Associated Abnormalities
-
Calculated PaCO2
- Useful in High Anion Gap Metabolic Acidosis
- Defines concurrent respiratory abnormalities
-
Excess Anion Gap
- EAG > 30 mEq/L: Metabolic Alkalosis present
- EAG < 23 mEq/L: Metabolic Acidosis present
VII. Resources
VIII. References
- Ghosh (2000) Fed Pract p. 23-33
- Killu and Sarani (2016) Fundamental Critical Care Support, p. 93-114
- Rutecki (Dec 1997) Consultant, p. 3067-74
- Rutecki (Jan 1998) Consultant, p. 131-42
- Arieff (1993) J Crit Illn 8(2): 224-46 [PubMed]
- Narins (1982) Am J Med 72:496 [PubMed]
- Narins (1980) Medicine 59:161-95 [PubMed]