
II. Definitions
- Bellow Failure
- Respiratory "pump" failure to expand chest and trigger inspiration
- Due to insufficient effort or respiratory drive, neuromuscular Impairment, muscle Fatigue, inefficient bellows
III. Background
- Respiratory Failure represents a loss of the normal, substantial Ventilatory reserve
- In those without Bellows Failure, Minute Ventilation may increase 20 fold over a baseline of 6 l/min
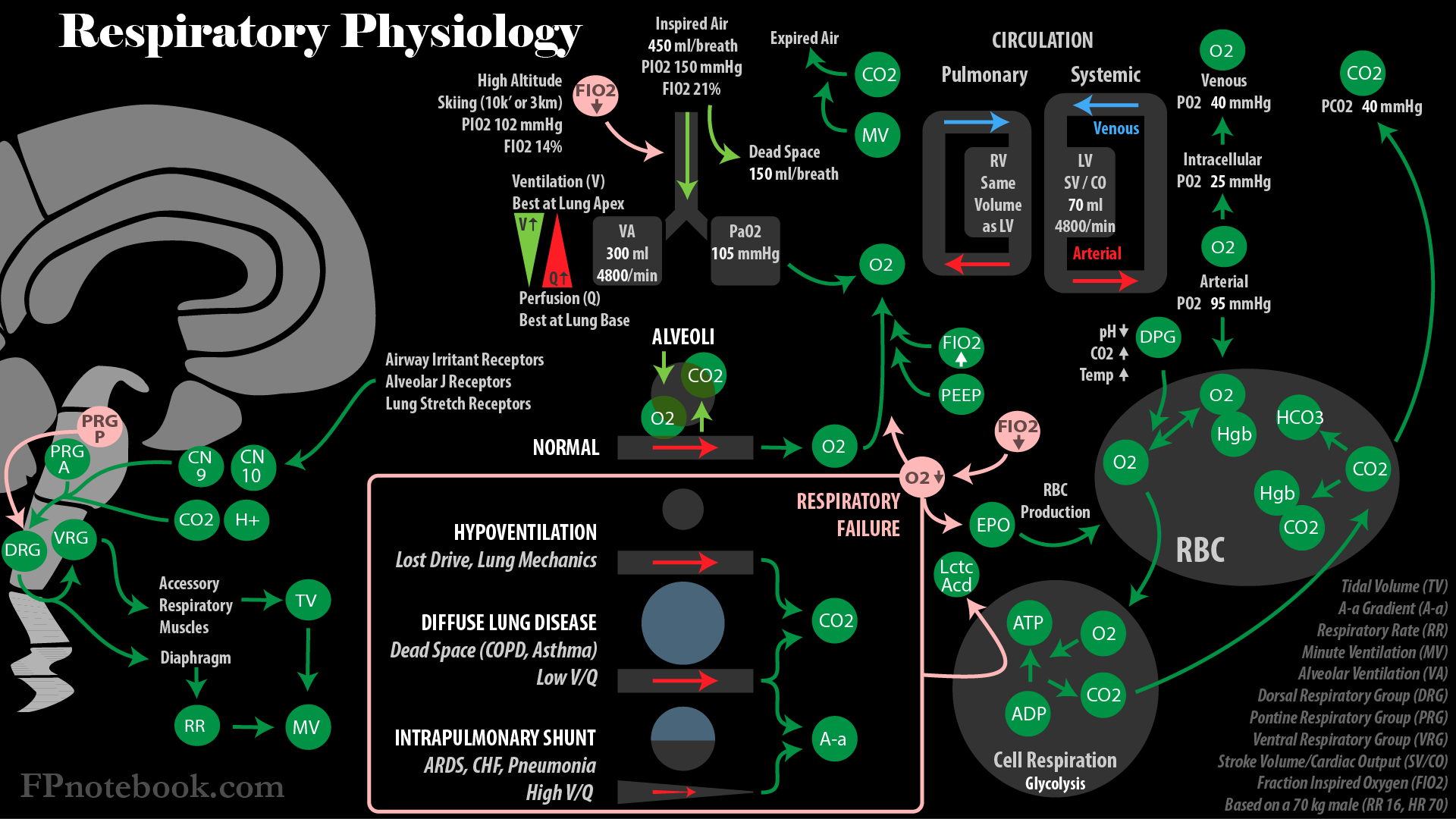
- Images
IV. Types: Hypoventilatory Respiratory Failure with Hypercapnia due to Bellows Failure
- Defining features
- High PaCO2 >50 mmHg
- Normal A-a Gradient
- Contrast with decompensated COPD in which pCO2 is increased, but A-a Gradient is high
- Normal A-a Gradient suggests external cause, with normal lungs and normal alveolar gas exchange
- Causes: Compromised lung mechanics
- Background
- Work of breathing costs increase significantly with impaired lung mechanics
- Patients with normal lungs expend only 1 ml oxygen per 1 liter of Minute Ventilation
- Patients with impaired lungs may expend 10-20 ml oxygen per 1 liter of Minute Ventilation
- Respiratory Muscles Fatigue and fail at acute, persistent workloads >40% of maximal workload
- Upper airway obstruction
- Pulmonary muscle Fatigue (Skeletal muscle Fatigues at >40% of maximum load)
- Obesity
- Supine position
- Kyphoscoliosis
- Ankylosing Spondylitis
- Hypercarbia (fever, Sepsis, burns)
- Inefficient breathing
- Obstructive Lung Disease (flat diaphragm, high Residual Volume)
- Restrictive Lung Disease
- Anatomic Dead Space accounts for a large percentage of a fixed, reduced Tidal Volume
- Chest Trauma
- Pneumothorax
- Air in the pleural space prevents negative pressure from forming within the chest
- Loss of negative pressure results in lung failing to expand with diaphragmatic excursion
- Flail Chest or multiple Rib Fractures
- Diaphragmatic Rupture
- Hemothorax
- Pneumothorax
- Other chest conditions interfering with ventilation
- Background
- Causes: Loss of Inspiratory Drive (Insufficient Effort)
- Drug Overdose or depressant drugs
- Brainstem injury
- Severe global CNS injury
- Head Trauma
- Intracranial Hemorrhage
- CNS Infection (Meningitis, Encephalitis, Brain Abscess, West Nile Encephalitis, Poliomyelitis)
- Central Sleep Apnea
- Central Alveolar Hypoventilation Syndrome (CHS)
- CO2 Retention
- Blue Bloaters (Chronic Bronchitis)
- Obese with hypoventilation despite Hypoxia
- Hypercarbia resulting in increased sedation
- Cyanotic (polycythemic with increased desaturated Hemoglobin)
- Blue Bloaters (Chronic Bronchitis)
- Causes: Neuromuscular
- Toxins (or other medication adverse effects)
- Electrolyte and endocrine abnormalities
- Nerve dysfunction
- Cervical Spine Injury
- Polyneuritis (e.g. Guillain-Barre Syndrome)
- Amyotrophic Lateral Sclerosis
- Multiple Sclerosis
- Nerve Agent Exposure (e.g. Organophosphates)
- Phrenic nerve injury
- Muscular dysfunction
- Prolonged Mechanical Ventilation (see Ventilator Weaning)
- Congenital Muscular Dystrophy
- Myasthenia Gravis
- Polymyositis
- Tetanus
V. Types: Hypercarbic Respiratory Failure from Diffuse Severe Lung Disease (large Respiratory Dead Space)
- Background
- Severe, diffuse lung disease with poor gas exchange
- pCO2 is easily excreted even through mild-moderately disease alveoli
- Hypercarbia requires apnea (Bellows Failure) or diffuse, severely impaired gas exchange
- Ventilated lung with poor gas exchange is dead space, wasted ventilation
- Perfusion to lung units that receive less ventilation results in blood retaining more CO2 and less O2
- Increased respiratory effort cannot fully compensate for increased dead space and CO2 production
- Severe, diffuse lung disease with poor gas exchange
- Defining features
- High PaCO2
- May be normal or low in mild to moderate disease compensated with Hyperventilation
- However, with decompensation, pCO2 rises
- Low PaO2
- Increased A-a Gradient
- Often improves with Supplemental Oxygen
- High PaCO2
- Causes:
- Decompensated Obstructive Lung Disease
- Asthma or Bronchospasm
- Chronic Obstructive Pulmonary Disease (COPD)
- Decompensated Interstitial Lung Disease (e.g. Idiopathic Pulmonary Fibrosis, Sarcoidosis)
- Decompensated Cystic Fibrosis
- Decompensated Obstructive Lung Disease
VI. Types: Hypoxemic Respiratory Failure without Hypercarbia from Intrapulmonary Shunting
- Background
- Alveoli fill with fluid (esp. in dependent lung) and are unable to oxygenate
- Interstitial fluid results in stiff lungs that ventilate poorly
- Small airways collapse
- Right to Left intrapulmonary shunt past poorly ventilated lung
- Carbon dioxide may still be expired as dead space is not increased (contrast with hypercapnic failure)
- CO2 is highly soluble in fluid (contrast with O2) and diffuses well despite fluid filled alveoli
- Patient cannot oxygenate despite increased Respiratory Rate and ventilation
- Blood in non-edematous lung is fully saturated with oxygen
- Blood in edematous lung is not able to oxygenate
- Defining features
- Low PaCO2
- Contrast with Bellows Failure and Decompensated Severe, Diffusely impaired alveolar gas exchange
- Low PaO2 <50-60 mmHg on room air
- A-a Gradient may be increased
- May not improve with Supplemental Oxygen
- Low PaCO2
- Causes: Improved with Supplemental Oxygen
- Causes: Not improved with Supplemental Oxygen (pO2 <50 mmHg despite oxygen)
- Suggests Physiologic right to left intrapulmonary shunting (esp. lung edema)
- Oxygen and Hyperventilation are unable to compensate for shunted (non-oxygenated) blood
- Blood has a fixed ceiling for Oxygen Saturation, above which no further oxygen is absorbed
- pO2 increases with FIO2 and alveolar recruitment from diseased, shunted regions
- Alveolar recruitment increases with NIPPV (PEEP, CPAP, BiPAP) and Mechanical Ventilation
- Cardiac Pulmonary Edema (increased transcapillary pressure)
- Left Ventricular Failure
- Acute Myocardial Ischemia (left ventricle)
- Malignant Hypertension
- Mitral Regurgitation or stenosis
- Lung Conditions (often with increased capillary permeability)
- Severe Lobar Pneumonia
- Pulmonary Contusion
- Diffuse Alveolar Hemorrhage
- Acute Respiratory Distress Syndrome (ARDS)
- Increased permeability (low pressure edema)
- Suggests Physiologic right to left intrapulmonary shunting (esp. lung edema)
VII. Types: Miscellaneous Secondary Causes of Hypoxia
VIII. Symptoms
- Moderate to Severe Dyspnea
- Altered Mental Status
IX. Signs
-
General appearance
- Altered Mental Status
- Diaphoresis
- Increased work of breathing
- Cardiovascular changes
- Mucous membrane and nail bed Cyanosis
- Tachycardia
- Hypertension
X. Labs
- Complete Blood Count
- Comprehensive Metabolic Panel
- Serum Troponin
- Serum Brain Natriuretic Peptide (BNP, NT-proBNP)
- D-Dimer
-
Arterial Blood Gas (or Venous Blood Gas)
- See ABG Interpretation
- Venous Blood Gas (VBG) is often used instead, but cannot use pO2 based calculations (e.g. A-a Gradient)
- A-a Gradient
- Distinguishes intrinsic lung causes (e.g. V/Q mismatch) from external causes (e.g. Bellows Failure)
- Increased A-a Gradient suggests intrinsic lung cause, whereas A-a Gradient is normal in external causes
- Increased pCO2 Causes (>45 mmHg)
- Bellows Failure with inadequate ventilation (normal lungs and gas exchange)
- Normal A-a Gradient
- Severely abnormal lungs with V/Q mismatch and unable to compensate with Minute Ventilation (e.g. COPD)
- Increased A-a Gradient
- Bellows Failure with inadequate ventilation (normal lungs and gas exchange)
- Other findings
- Respiratory Acidosis with pH <7.35
- Hypoxia with (PaO2/FIO2 Ratio <300 mmHg)
XI. Imaging
XII. Differential Diagnosis
- See Causes above
- See Dyspnea Causes
- See Tachypnea Causes
- See Hypoxia
XIII. Management: General
- See Emergency Breathing Management
- See Advanced Airway
- See Non-Invasive Positive Pressure Ventilation
- See Mechanical Ventilation
- Specific Approaches
XIV. Management: Bellows Failure or apnea
- Findings: Increased PaCO2, normal A-a Gradient
- Aggressive management is required (e.g. consider Endotracheal Intubation and Mechanical Ventilation)
- Manage immediately reversible causes (e.g. coma cocktail with Naloxone, dextrose)
- Consider upper airway obstruction (e.g. Anaphylaxis, Foreign Body Aspiration)
- Evaluate Trauma patients for chest wall defects interfering with bellows function (e.g. Flail Chest)
- Evaluate for impending Respiratory Failure (e.g. Guillain Barre Syndrome, Myasthenia Gravis)
- Single Breath Counting <10 to 15
- Vital Capacity <15-20 ml/kg
- Tidal Volume <5 ml/kg
- Maximum expiratory force <40 cm H2O (normally >100 cm H2O)
- Maximum inspiratory pressure less negative than -30 cm H2O (normally < -100 cm H2O)
XV. Management: Hypercarbic Respiratory Failure from Diffuse Severe Lung Disease (large Respiratory Dead Space)
-
COPD
- See Emergency Management of COPD Exacerbation
- Conservative management with controlled Oxygen Delivery (avoiding CO2 narcosis)
- Bronchodilators and Corticosteroids
- Non-Invasive Positive Pressure Ventilation (NIPPV) as needed
- Antibiotics for productive or purulent cough and increased Dyspnea or requiring NIPPV or Intubation
- Comorbid Right Heart Failure may Compound Presentation
- Avoid Endotracheal Intubation and Mechanical Ventilation if possible
- Ventilator Weaning may be more difficult
- See Mechanical Ventilation for settings
- Requires larger Tidal Volumes (e.g. 10 ml/kg) due to large Physiologic Dead Space
- Avoid excessive correction of PaCO2
- Correct pH, but avoid Respiratory Alkalosis
- Allows for pre-existing metabolically compensated hypercarbia
- Decrease air trapping by allowing greater time for expiration
- Shorten inspiratory time by increasing inspiratory rate
- Decrease Respiratory Rate
-
Asthma
- See Emergency Management of Asthma Exacerbation (or Status Asthmaticus)
-
Asthma Exacerbations are acute and reversible, and Dyspnea is always present (otherwise similar to COPD)
- Severe V/Q mismatch with wasted gas exchange and compensatory increased Minute Ventilation
- Airflow obstruction with hyperinflation results in increased work of breathing and muscle Fatigue
- Unlike COPD, most Asthma Exacerbations are without PaCO2 rise
- PaO2 is typically only mildly decreased and PaCO2 is typically low (not hypercarbic)
- Frequent Bronchodilators, initiate Corticosteroids (delayed effect), and manage Asthma triggers
- Very Severe Asthma Exacerbation (Status Asthmaticus) is associated with Respiratory Failure
- See Status Asthmaticus
- Emergent management with continuous Bronchodilators, Epinephrine, Magnesium, NIPPV
- Beta Agonists are less effective in acidosis, with worsening response to maximal therapy
- Increased PaCO2 >40 mmHg is a harbinger of impending respiratory arrest
- Endotracheal Intubation if acute aggressive management of airway obstruction fails
-
Endotracheal Intubation and Mechanical Ventilation
- Unlike weaning in COPD, asthma Ventilator Weaning is more simple
- Patients tolerate removal of Mechanical Ventilation when acute airway obstruction resolves
- Management is challenging due to hyperinflation
- High pressures are required to provide even adequate Tidal Volume
- As with COPD, decrease air trapping by allowing greater expiration time
- Shorten inspiratory time by increasing inspiratory rate
- Decrease Respiratory Rate (requires adequate sedation)
- Allow for mild hypercarbia and Respiratory Acidosis
- PaCO2 need not be <40 mmHg
- pH>7.20 is sufficient
- Unlike weaning in COPD, asthma Ventilator Weaning is more simple
XVI. Management: Intrapulmonary Shunting (Pulmonary Edema, Lung Consolidation)
-
Acute Respiratory Distress Syndrome (ARDS or noncardiac Pulmonary Edema)
- See Acute Respiratory Distress Syndrome
- Typically a previously healthy patient with serious triggering event (e.g. Trauma, Sepsis)
- Trigger causes diffuse alveolar-capillary membrane injury with increased permeability
- Protein rich fluid extravasates from capillaries and floods the alveoli
- Alveoli are without ventilation, but still perfused
- Presents with Dyspnea, Tachypnea, Tachycardia with diffuse interstitial lung edema (and no Peripheral Edema)
- Oxygenation
- Provide adequate Supplemental Oxygen
- Avoid excessive oxygen which is toxic to damaged lung alveoli
- Supportive Care
- See Acute Respiratory Distress Syndrome for full supportive measures
- Conservative IV hydration to prevent Fluid Overload
- Excess intravascular fluid increases hydrostatic pressures at alveolar capillary, increased Pulmonary Edema
- Maintain adequate Cardiac Output but keep Central Venous Pressures and Wedge Pressure lower
- Treat the underlying condition that triggered ARDS
- Beta Agonists and consider Corticosteroids
- Antibiotics for primary and secondary infections
- Body position changes (prone)
- Consider ECMO
- Mechanical Ventilation: Lung Protective strategy (limit Barotrauma)
- Start with low Tidal Volumes (e.g. 6 ml/kg based on Ideal Body Weight)
- Lower FIO2 to avoid alveolar toxicity
- Adjust Positive End Expiratory Pressure (PEEP) in step with FIO2 (See PEEP Table)
- Allow some hypercapnia to reduce Barotrauma risk (permissive hypercapnia)
- Lower minute volumes (lower Tidal Volume and rate)
- Titrate to pH of 7.20 to 7.30, PaCO2 up to 50 mmHg (permissive hypercapnia)
-
Cardiogenic Pulmonary Edema
- See Congestive Heart Failure Exacerbation Management
- Similar pathophysiology to ARDS, despite the different underlying cause
- Unlike ARDS, Hypoxemia may respond rapidly to emergent management (BiPaP, high dose IV Nitroglycerin, diuresis)
- However, if Hypoxemia is refractory, Mechanical Ventilation is effective at improving oxygenation
- Cardiogenic Shock tolerates poorly the increased work of breathing, and Ventilator may unload workload
- Lobar Bacterial Pneumonia
- See Pneumonia Management
- Intrapulmonary shunting due to Lung Consolidation
- Presenting with fever, Pleuritic Chest Pain, Purulent Sputum, Tachycardia, Tachypnea and dense Alveolar Infiltrate
- As with other intrapulmonary shunting, Hypoxemia (low PaO2) with low PaCO2 is typical
- Response to Supplemental Oxygen is poor, except in regions of poor ventilation (low V/Q)
- Supplemental Oxygen does not compensate for intrapulmonary shunt
- Hypoxemia is worsened by concurrent Septic Shock with lower mixed venous PO2
- Correction of shock state may improve oxygenation by raising venous PO2
- Response to Supplemental Oxygen is poor, except in regions of poor ventilation (low V/Q)
- Positioning
- Positioning of good lung down, favors perfusion to the lung better able to ventilate
- Mechanical Ventilation
- Consider in Unstable Patients, unable to sustain high work of breathing
- Oxygenation may remain poor despite Mechanical Ventilation
- Exercise caution with PEEP
XVII. Management: Approach to Non-Invasive Positive Pressure Ventilation Selection
- Hypoxemic Respiratory Failure (Inadequate oxygenation)
- Reflected by Arterial Blood GasPaO2 and Oxygen Saturation
- Concepts
- Increase oxygen delivered to the lung (esp. FIO2) or
- Increase mean airway pressure (or Positive End-Expiratory Pressure)
- Interventions
- Hypercarbic Respiratory Failure (Inadequate ventilation)
- Reflected by Arterial Blood GasPaCO2 and pH
- Concepts (increase Minute Ventilation)
- Increase Tidal Volume (TV) or
- Increase Respiratory Rate (RR)
- Interventions
- References
- Mallemat and Runde in Herbert (2015) EM:Rap 15(2): 7-8
XVIII. References
- (2016) Fundamental Critical Care Support, p. 46-60
- Davies (1986) Acute Respiratory Failure, Cyberlog
- Presberg in Noble (2001) Primary Care, p. 705-16