
II. Pathophysiology
- See Ketoacidosis
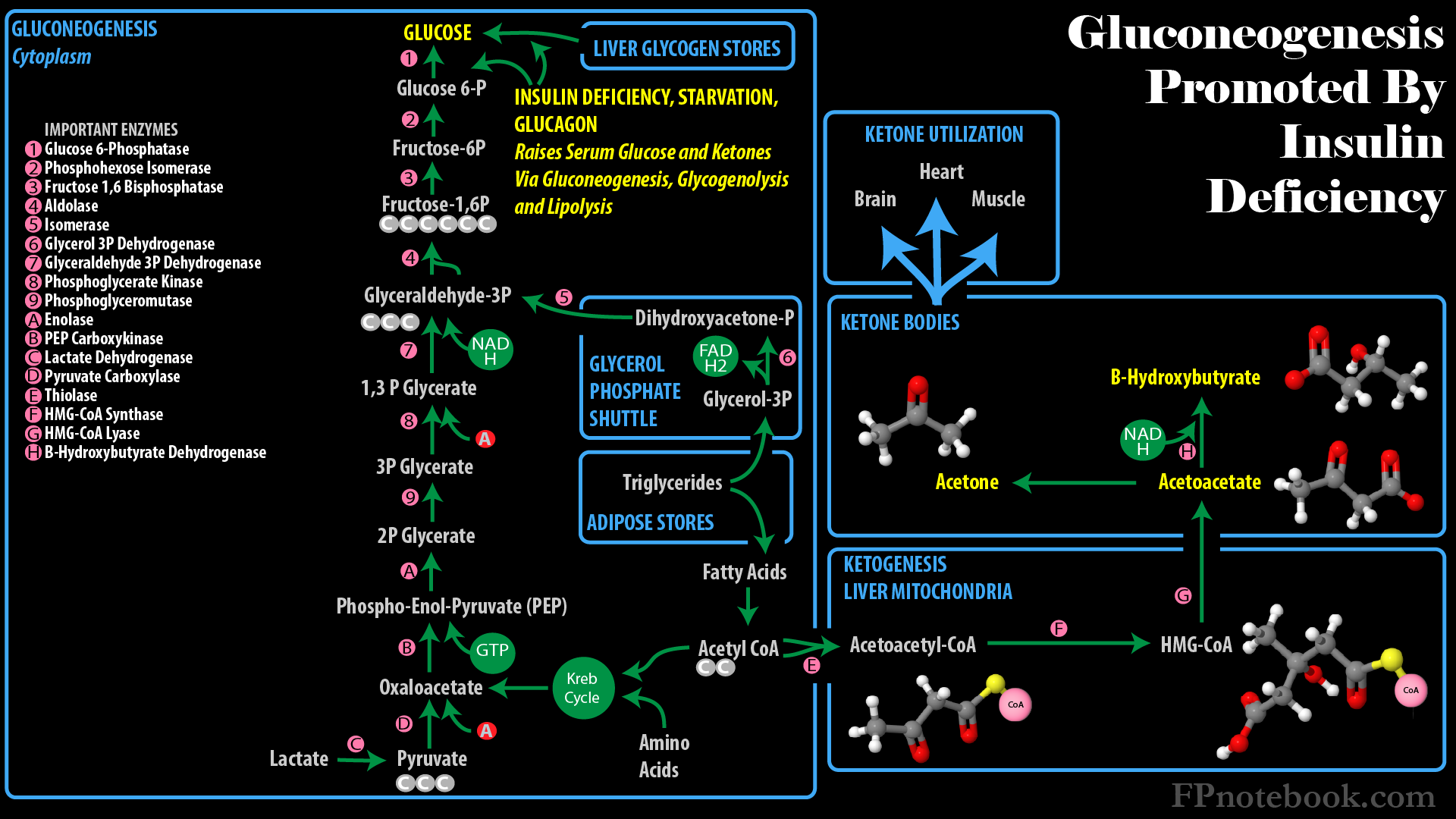
- See Glucose Metabolism
- Develops in baseline chronic Alcohol Abuse and associated poor nutrition, in combination with an acute stressor
- Identifying the acute stressor is key to effective management (see causes below)
- Most common triggers are infection and Pancreatitis
- Often occurs with recent Alcohol cessation
-
Alcoholism results in reduced glycogen and nutritional stores (starvation state)
- Occurs when most of daily calories are obtained from Alcohol
- Ethanol is a 2 carbon Alcohol that cannot be burned as fuel in the TCA Cycle, nor used for Gluconeogenesis
- Ethanol can only be metabolized to Ketone Bodies for fuel, or used to build Fatty Acids and Triglycerides
- Contrast with Glycolysis and Gluconeogenesis pathways, dependent on 3-carbon sugars (e.g. pyruvate)
- Glucose is depleted by decreased Gluconeogenesis and glycogenolysis
- Compounded by advanced liver disease, in which hepatic Gluconeogenesis is impaired
- Initial response to starvation is to increase hormonal factors that transiently increase Glucose levels
- These factors include Glucagon, Catecholamines, Cortisol and Growth Hormones
- Ketoacidosis results from increased lipolysis and Ketone generation when Glucose is unavailable
- Alcohol is metabolized to Ketones by hepatic Alcohol dehydrogenase
- Fatty Acids are also metabolized to Ketones for energy utilization
- Lactic Acidosis also develops
- Alcohol metabolism increases NADH to NAD+ ratio and a suppression of mitochondrial activity
- Lactic Acid accumulates with disrupted mitochondrial activity (pyruvate is unable to enter TCA Cycle)
- Lactic Acid further increases in advanced liver disease with impaired Gluconeogenesis
- Volume depletion (Dehydration) is frequently also present and compounds the Lactic Acidosis
- Occurs when most of daily calories are obtained from Alcohol
- Images
III. Causes
- Intraabdominal Disorder
- Other Alcohol related disorder
- Other metabolic disorder
- Other Systemic Disorders
- Toxic Ingestion
- Salicylate Toxicity
- Toxic Alcohol Ingestion (e.g. Ethylene Glycol Poisoning)
IV. Symptoms
- Nausea and Vomiting (frequently with volume depletion)
- Generalized Abdominal Pain
V. Signs: Red Flags
- Significant intraabdominal findings suggest a possible underlying trigger (see causes above)
- Peritoneal signs
- Abnormal bowel sounds
- Abdominal Distention or significant tenderness
- Significant Altered Level of Consciousness (expect only mild alteration in Alcoholic Ketoacidosis)
- See Altered Level of Consciousness
- Consider Unknown Ingestion (coingestion)
- Consider Wernicke Encephalopathy
- Toxic Alcohol Ingestion (e.g. Ethylene Glycol Poisoning)
- Consider in severe Lactic Acidosis, Altered Mental Status, Osmolal Gap
VI. Labs
- Comprehensive Metabolic Panel
- Increased Anion Gap
- Decreased serum bicarbonate
- Serum Glucose is typically low or normal (elevated in 10% of cases)
- Other Electrolyte abnormalities may be present
- Serum levels are unreliable in evaluating total body stores (esp. Phosphorus, Magnesium)
- Hyponatremia
- Hypomagnesemia
- Hypokalemia
- Hypophosphatemia
-
Venous Blood Gas
- Metabolic Acidosis
- Mixed acid base findings are common (75% of cases)
-
Serum Ketones
- Increased Beta Hydroxybutyrate in addition to other Ketones
- Ketones are elevated more than Lactic Acid in uncomplicated Alcoholic Ketoacidosis
- Serum Lactate
- Lactic Acid is mildly elevated (rarely >4 mmol/L) in uncomplicated Alcoholic Ketoacidosis
- Significantly increased (>4 mmol/L) in Toxic Alcohol ingestion (Methanol or Ethylene Glycol Poisoning)
-
Osmolar Gap
- Consider Toxic Alcohol ingestion (Methanol or Ethylene Glycol Poisoning)
- Serum Alcohol Level
- Alcohol level is independent to Ketoacidosis development (may be high or low)
-
Toxicology Screening
- Consider other causes of Metabolic Acidosis with Anion Gap (e.g. Salicylism, Toxic Alcohols, Rhabdomyolysis)
VII. Management
- Similar to Starvation Ketosis
- Most common cause of Metabolic Acidosis with Anion Gap in Alcoholics (poor nutrition)
- However, exclude Toxic Alcohol ingestion (e.g. Ethylene Glycol Poisoning)
- As with Diabetic Ketoacidosis, Serum Beta Hydroxybutyrate is increased
- Urine Ketones are unreliable for detection
- Administer IV fluids containing dextrose (e.g. D5LR)
- Emergent correction of Hypoglycemia (Serum Glucose <60 mg/dl)
- Before dextrose, give Thiamine 200 mg IV (500 mg IV if Wernicke Encephalopathy suspected)
- Dextrose infusions stop Ketone formation, whereas simple crystalloid will not
- However, assess Potassium and replace before significant dextrose aministered (Hypokalemia risk)
- Anticipate Ketone clearance and acidosis resolution within 8 to 12 hours of starting fluid and dextrose infusion
- Replace other Electrolytes as needed
- Alcoholism Management
VIII. References
- Long and Swaminathan in Swadron (2022) EM: Rap 22(9): 13-5
- Thorson and Abboud (2024) Crit Dec Emerg Med 38(7): 16-7