
II. Definitions
- Penetrating Neck Trauma
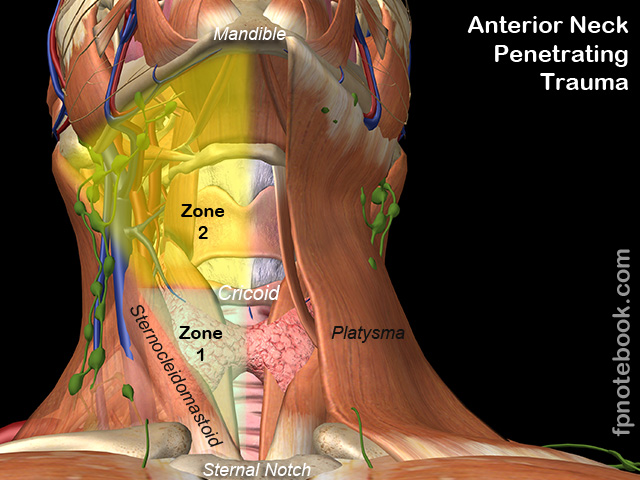
- Injury with penetration of the platysma Muscle
III. Precautions
- First priorities in Penetrating Neck Trauma are Airway and Vascular Injury
- See ABC Management
- Assume a dynamic airway
- Neck Hematomas and subcutaneous edema increase over time
- Reassess the airway frequently for developing obstruction
- Do not be distracted by the actual neck wound
- Hold pressure on the wound and complete the Trauma survey
IV. Symptoms
- Dysphagia
- Hoarseness
- Bleeding from nose or mouth
- Neurologic deficit
- Hypotension
V. Signs
- Subcutaneous Emphysema
- Stridor
- Respiratory distress
- Expanding Hematoma
- Active bleeding from wound site
- Carotid Bruit
- Loss of pulse
- Neurologic deficit
- CNS findings may be due to ischemia
- Unilateral motor deficits or dermatomal sensory changes (consider nerve injury proximal to the Brachial Plexus)
VI. Exam: Wound Evaluation
- Clean blood from wound
- Determine if platysma was breached (if possible)
- Estimate wound depth and trajectory based on observation
- Avoid probing neck wounds to determine depth
VII. Exam: Localization of underlying injuries
- Determine depth of penetrating injury
- Determine anterior triangle or posterior triangle injury
- Anterior triangle (Anterior to sternocleidomastoid)
- Most major structures (major vessels, trachea, Esophagus)
- Posterior triangle (Posterior to sternocleidomastoid)
- Spinal Column (rare injury from Spinal Trauma)
- Images
- Anterior triangle (Anterior to sternocleidomastoid)
- Determine Zone of injury (Zone 1 inferiorly to Zone 3 superiorly)
- Precautions
- Most neck injuries are not limited to one zone
- Patients have typically been stabbed multiple times
- Neck wounds (esp. Gunshot Wounds) typically cut across neck zones
- Injury zones play a reduced role in current day Penetrating Neck Trauma
- As of 2013, evaluation is exam-based with CT Angiography
- See evaluation protocol below
- Injury zones were originally developed to risk stratify patients based on ease of surgical exploration
- Zone 2 injuries are less difficult to explore than Zone 1 and 3
- Zone 2 Penetrating Trauma was typically explored in OR
- Resulted in a large number of unnecessary explorations
- Zone 1 and 3 Penetrating Trauma evaluation is more difficult
- Typically required complicated evaluation protocols including standard angiogram
- Most neck injuries are not limited to one zone
- Zone 1 (sternal notch to cricoid ring/clavicle head)
- Lung apex (injury results in Pneumothorax, Hemothorax)
- Common Carotid Artery
- Subclavian artery
- Vertebral Artery
- Zone 2 (cricoid ring to angle of Mandible) - Highest risk region (but most accessible to exploration)
- Internal Carotid Artery
- Internal Jugular Vein
- Sympathetic trunk (injury results in Hypotension)
- Recurrent laryngeal nerve (injury results in Hoarseness)
- Trachea
- Larynx
- Esophagus
- Zone 3 (angle of Mandible to skull base)
- Vertebral Artery
- External Carotid Artery
- Precautions
- Determine trajectory
- Penetrating injury toward vital structures (e.g. medial trajectory) or
- Penetrating injury away from vital structures (e.g. lateral trajectory)
VIII. Evaluation
- Immediate surgery indications (hard signs of serious injury)
- Arterial injury
- Cerebral ischemia (e.g. new Hemiplegia suggesting carotid injury)
- Unstable Patient with shock assumed secondary to neck Trauma
- Expanding or pulsatile Hematoma
- Severe active bleeding (pulsatile bleeding, arterial bleeding)
- Refractory shock state
- Radial Pulse diminished or absent on the side of injury
- Arterial Bruit or thrill
- Aerodigestive injury (less common)
- Airway obstruction
- Hemoptysis
- Hematemesis
- Wound with air bubbling through
- Arterial injury
- Intermediate or Soft Signs (platysma penetration without hard signs)
- Soft Sign Indications
- Stable neck Hematoma
- Hoarseness
- Dysphagia
- Mild subcutaneous Emphysema
- Minor Hematemesis
- Minor Hemoptysis
- CT Angiography of Neck in most patients
- Consult with Trauma surgery for local protocols
- Soft Sign Indications
- Asymptomatic Patients (no hard or soft signs) AND no platysma penetration
- Close neck wound
- May discharge home if no complications on serial examination
- CT Angiography of Neck based decision making
- Obvious CTA abnormalities requiring operative management
- Immediate surgery
- Intermediate CTA findings (possible aerodigestive injuries): Options for evaluation
- Bronchoscopy
- Laryngoscopy
- Upper endoscopy
- Barium Swallow
- Endovascular intervention (e.g. posterior vascular injury, such as Vertebral Artery injury)
- No obvious CTA abnormalities to indicate immediate surgery
- Consult local Trauma surgery for recommendations
- Penetration trajectory toward vital structures
- Admit for observation
- Penetration trajectory away from vital structures
- Observe for 6-12 hours
- May discharge if stable following observation
- Obvious CTA abnormalities requiring operative management
IX. Management
- General
- Alert Trauma surgery as early as possible
- If no Trauma surgery available at facility, arrange emergent transport
- Defer imaging to the receiving facility if no means to manage findings at initial site
-
Cervical Spine Immobilization indications
- Neurologic deficit
- Altered Level of Consciousness
- Bleeding control
- Apply direct pressure (firmly with fingers, not an inserted gauze wad)
- Avoid removing A bandage if adequate control (esp. if heavier or pulsatile bleeding prior to bandage)
- Do not clamp due to significant risk of collateral damage
- Bleeding refractory to pressure
- Consider inserting a foley into wound and inflating with saline
- Consider initiating Massive Transfusion Protocol early
- Venous access
- Obtain on opposite side of injury
- Patient cooperation may be difficult due to anxiousness, airway compromise
-
Advanced Airway management (intubation, Cricothyrotomy)
- See Advanced Airway for general indications
- Absolute indications for Advanced Airway
- Decreased mental status
- Expanding Hematoma
- Tracheolaryngeal injury (Tracheal Tear, Laryngeal Fracture)
- Hypoxia
- Hypoventilation
- Additional indications to consider for Advanced Airway
- Interhospital transfer
- Risk of progressive airway compromise
- Early Advanced Airway placement is preferred if risk of progression
- Technique
- Rapid Sequence Intubation
- Video Laryngoscopy or Fiberoptic intubation over bronchoscope if available
- Consider double set-up for immediate Cricothyrotomy as a backup plan
- Use slightly smaller Endotracheal Tube than typically used (e.g. decrease by 1/2 size)
- Exposed trachea may be intubated directly over a bougie
- Avoid blind techniques (risk of exacerbating airway injury)
- Avoid Extraglottic Devices (e.g. LMA, Combitube)
- Avoid Nasotracheal Intubation
X. References
- (2008) ATLS Manual, American College of Surgeons
- Birnbaumer in Herbert (2012) EM:Rap 12(10): 9-11
- Cowling and Bernard (2024) Crit Dec Emerg Med 38(2): 4-10
- Inaba and Spangler in Herbert (2016) EM:Rap 16(11): 5
- Inaba and Herbert in Hebert (2013) EM:Rap 13(3): 7
- Swaminathan and Hicks in Herbert (2019) EM:Rap 19(1): 12-3, 15-6