
II. Epidemiology
- Common in Atomic bomb survivors
- Peak Incidence at ages 30 to 50 years old
III. Pathophysiology
- Chronic phase (Mild, indolent course)
- Excessive Granulocyte (Neutrophils) proliferation
- Blastic phase (Malignant, leukemic course)
- Increased blasts and Promyelocytes
IV. Symptoms
- Asymptomatic in 20% of patients
- Weakness
- Hypermetabolism
- Weight loss
- Fever
- Arthralgias
- Bone pain
- Excessive bleeding (spontaneous or with surgery)
V. Signs
VI. Labs
- Philadelphia Chromosome (BCR-ABL1 Fusion Gene)
- Present in 90 to 95% of CML cases on peripheral blood or Bone Marrow testing
- Also present in ALL (2-4% of children, 20-40% of adults)
- Reciprocal Chromosome translocation
- Long arm of Chromosome 22 (c-sis Oncogene)
- Long arm of Chromosome 9 (c-abl Oncogene)
- Translocation of C-abl at bcr breakpoint
- Forms bcr/abl
- Present in 90 to 95% of CML cases on peripheral blood or Bone Marrow testing
-
Complete Blood Count
- Chronic Phase
- White Blood Cell Count > 200,000/uL
- Granulocytes (especially Neutrophils) predominate
- Transitional Phase (50% of patients)
- Blast Phase
- Increased Leukocytosis
- Thrombocytosis
- Chronic Phase
-
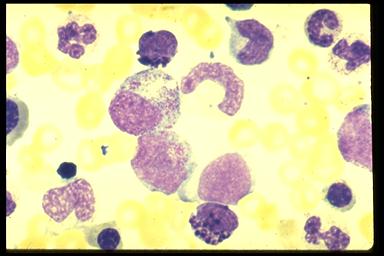
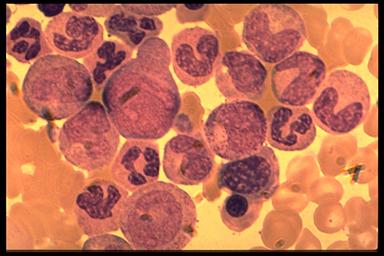
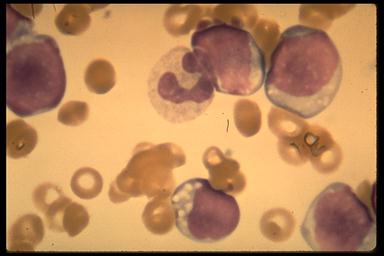
Bone Marrow Biopsy and Peripheral Smear
- Chronic Phase
- Myeloblasts represent <5% of cells
- Blast Phase
- Large proportion of immature cells
- Images
- Chronic Phase
- Other Findings
- Vitamin B12 markedly elevated
- Leukocyte Alkaline Phosphatase reduced
- Uric Acid increased
VII. Management: CML Treatment
- Treatment for cure
- Allogeneic Stem Cell Transplant (SCT)
- Chronic Phase suppression
- First Line
- Tyrosine Kinase Inhibitor: Imatinib (Gleevac)
- Gleevac is generic in U.S. as of February 2016
- Monitor for complications (thrombotic events, CV and GI complications)
- Monitor CBC every 3 months
- Interferon-alfa with Cytarabine
- May be poorly tolerated
- Studies to date show unclear efficacy
- Tyrosine Kinase Inhibitor: Imatinib (Gleevac)
- Alternative (prior first line agents)
- Hydroxyurea (used to stabilize chronic phase)
- Busulfan
- Risk of myelosuppression
- Hydroxyurea is preferred
- Other Alkylating Agents (not in marrow transplant)
- Splenectomy rarely indicated
- Hypersplenism
- Repeated painful splenic infarctions
- Consider Bone Marrow Transplantation in first year
- Results in 70% long-term disease free survival
- First Line
-
Blast Crisis
- Often refractory to treatment
- Try protocols for Acute Lymphocytic Leukemia
VIII. Management: Surveillance of CML Survivors
-
Complete Blood Count (CBC) every 3 months
- Hematology Consultation for Neutropenia (ANC <1000/mm3) or Thrombocytopenia (Platelet Count <50k/mm3)
- Symptom surveillance
- Patients treated with Hematopoietic Stem Cell Transplantation
- See Hematopoietic Stem Cell Transplant for protocol
IX. Course
- Initially indolent
- Later progresses to leukemic phase (Blast Crisis)
- Blast phase onset after 6-12 months post diagnosis
- Annual progression to blast phase: 25% of patients
X. Prognosis
- Five year survival
- Age under 50 years old: 84% five year survival
- Age over 50 years old: 48% five year survival
XI. References
- (2001) Med Lett Drugs Ther 43(1106):49-50
- Druker in Abeloff (2004) Clinical Oncology p. 2899-915
- Enright in Hoffman (2000) Hematology 40:1155-67
- Davis (2014) Am Fam Physician 89(9): 731-8 [PubMed]
- Gbenjo (2023) Am Fam Physician 107(4): 397-405 [PubMed]