
II. Indications
- Airway maintenance
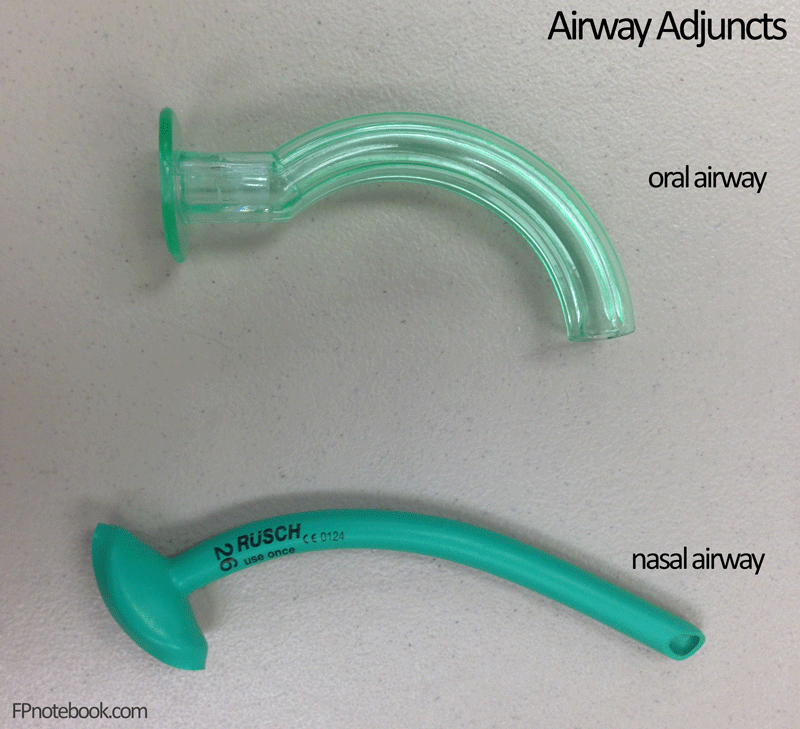
- Oral Airway placement difficult
- Semiconscious patient not tolerating Oral Airway
- Nasotracheal Intubation guide in Maxillofacial Trauma
III. Contraindications
- Facial injury
- Basilar Skull Fracture
- Coagulopathy
IV. Complications
- Esophageal intubation (if too long)
- Laryngospasm
- Vomiting (less likely than with Oral Airway)
- Nasal mucosa injury and secondary blood aspiration
V. Sizing
VI. Technique
- Lubricate with water soluble lubricant (or Anesthetic jelly)
- Gently insert into nostril
- Leading edge of bevel should be away from septum (away from Kiesselbach's Plexus)
- If results in upside-down Nasal Trumpet, rotate 180 degrees after passing the anterior nare
- Insert along floor of nostril, perpendicular to face
- If resistance occurs
- Try slight tube rotation
- Try other nostril
- Leading edge of bevel should be away from septum (away from Kiesselbach's Plexus)
- Check for respirations following placement
VII. Maintenance
- Check patency frequently
- Tube may be blocked by mucus, blood, secretions