
II. Indications
- Medications causing tissue necrosis on extravasation or otherwise harmful via peripheral IV
- Large volume infusion required
- Hemodialysis
- Unobtainable or unreliable Intravenous Access
- Pulmonary artery pacing
- Invasive Monitoring
- Right Ventricular Filling Pressures (Central Venous Pressure) and oxygenation (ScvO2)
- Left ventricular filling pressure (pulmonary artery catheter or wedge pressure)
III. Contraindications: General
- Patient refusal
- Uncooperative or agitated despite sedation
- Deep Vein Thrombosis in affected vessel
- Overlying skin abnormality or distorted anatomy
- Prior radiation or surgery distorting or scarring insertion site
- Inability to lie in Trendelenburg position (IJ, SVC; consider Femoral Line instead)
- Contralateral Pneumothorax (IJ, SVC; place on same side as Pneumothorax)
- Ipsilateral AV graft (e.g. Hemodialysis fistula)
- Adequate alternatives are available (e.g. large bore peripheral IV)
IV. Contraindications: Significant Coagulopathy
- Precautions in CVC Placement for coagulopathic patients
- Use real-time POCUS guidance (observing the needle from skin to vessel entry)
- Compressible vessels are preferred
- Use the smallest bore needles
- Most experienced operator should perform the line placement
- Safe without reversal IF Compressible site (e.g. IJ, femoral vein inferior to inguinal ligament) AND
- PTT <1.5 x UpperLimitNormal
- INR <3.0 in patient on Warfarin
- Platelet Count >20k
- Antiplatelet agents (e.g. Clopidogrel)
- Direct Oral Anticoagulants (DOAC)
- Safe without reversal IF Non-Compressible Site (e.g. subclavian vein) AND
- PTT <1.5 x UpperLimitNormal
- INR <2.0 in patient on Warfarin
- Platelet Count >50k
- Serum Creatinine <6 mg/dl (or consider with DDAVP)
- References
- Rutherford (2025) Anatomy of Central Venous Access, Hospital Procedures Course, attended 9/12/2025
V. Risk Factors: Mechanical Complications of CVC Placement
- Inexperienced operator
- More than 3 attempts at line placement (RR 6)
- Extremes of weight (BMI <20 or BMI > 30)
- Dehydration
- Large catheters
- Coagulopathy (see above)
- Prior central venous catheter in the same vein
- References
- Rutherford (2025) Anatomy of Central Venous Access, Hospital Procedures Course, attended 9/12/2025
VI. Preparation
- Informed Consent (patient or surrogate)
- Confirm Identity (verbally and with ID Band, Name, DOB)
- Review Patient History
- Anticoagulants (e.g. DOAC, Warfarin, therapeutic Enoxaparin, Fondaparinux)
- Antplatelets agents (Aspirin, Platelet ADP Receptor Antagonist such as Clopidogrel)
- Review Patient Labs
- Platelet Count
- PT/INR and PTT
- Blood Urea Nitrogen (Uremia with high BUN causes Coagulopathy)
- Equipment
- Skin antiseptic (e.g. Chlorhexidine, Povidone-Iodine, see above)
- Lidocaine 1%, syringe and needle for injection
- Introducer needle, slip tip syringe for guide wire insertion
- Dilator
- Seldinger guide wire
- Scalpel (#11 Blade)
- Triple Lumen Catheter (flush each line with sterile saline)
- Ultrasound with high frequency linear probe (and sterile probe covers with sterile gel)
- Perform under dynamic Ultrasound guidance
- Advantages
- Confirms vessel location and patency
- Real-time confirmation of vessel cannulation
- Decreases the number of access attempts
- Decreases the time to central vein catheterization
- Decreases central access complication rate
- Probe orientation (transverse and longitudinal have similar success rates)
- Transverse probe orientation
- Base needle entry distance from Ultrasound probe based on target vessel depth
- At 45 degree angle, entry distance = depth (e.g. 2 cm depth, 2 cm distance)
- At 30 degree angle entry distance = 1.7 x depth (e.g. 2 cm depth, 3.4 cm distance)
- Follow the needle tip as it is advanced toward the target vessel
- Slide the transverse oriented probe with the needle as it approaches the vessel
- Losing track of the needle tip risks needle malpositioning (esp. too deep)
- Base needle entry distance from Ultrasound probe based on target vessel depth
- Longitudinal probe orientation (indicator toward provider)
- Allows for visualization of needle along entire course
- Start in transverse orientation to identify vein and compressibility, and then rotate 90 degrees
- Risk of probe sliding laterally off vein on onto artery (caution!)
- Transverse probe orientation
- Advantages
- Estimate catheter insertion depth
- Initial guidewire insertion: 20 cm is sufficient in adult
- Right internal Jugular Vein (or right subclavian): Height (cm)/10
- Left internal Jugular Vein (or left subclavian): Height (cm)/10 + 4 cm
- Perform under sterile conditions to reduce infectious complications (i.e. CLABSI)
- Hand Hygiene (Hand Washing immediately before procedure)
- Mask, cap, sterile gown and sterile gloves
- Everyone in room within vicinity of procedure should wear a cap and mask
- Skin Preparation
- Chlorhexidine (preferred)
- Scrubbed back and forth vigorously, and must dry for 3 minutes before skin puncture
- Includes Chloraprep (Chlorhexidine gluconate and Isopropyl Alcohol)
- Povidone-Iodine (Betadine)
- Must dry for 5 minutes before skin puncture
- Chlorhexidine (preferred)
- Large sterile drape to cover entire patient
- Antimicrobial Dressing at catheter insertion site
- Sterile transducer sleeve around Ultrasound probe and cord
- Line insertion pearls
- Use Ultrasound guidance (see above)
- Approach vessel from a shallow angle (e.g. 30 degrees, maximum of 45 degrees)
- Stabilize needle and syringe on entering skin to prevent too forceful and deep initial needle entry
- Once blood enters syringe, stabilize needle with 3 three fingers against patient and remove needle
- Prevents needle exiting vessel while removing syringe
- Alternatively, an angiocatheter large enough to pass guidewire may be used for initial vessel entry
- On passing seldinger guidewire, the curve in guidewire should be directed toward heart (midline)
- Dilator insertion should parallel the needle entry angle (typically shallow)
- Twist the dilator as it enters vessel to ease venous catheter insertion
- On confirmation of line placement, aspirate each line
VII. Approach: Site Selection in stabilized patients
- Precaution
- Site selection should avoid sites with overlying infection, altered anatomy, Trauma or distortion
-
General patient without other risk factors
- Internal Jugular Central Line is preferred (lowest risk site)
- Avoid Femoral Central Line overall (aside from codes) due to the highest rate of complications (DVT, infection)
- Consider alternatives to central access
- Morbidly obese
- Subclavian Central Line is preferred
- Internal Jugular Vein landmarks are typically difficult to localize in the morbidly obese
- Avoid femoral vein Central Line due to infection risk
-
Pneumothorax or Hypoxemia
- Internal Jugular Central Line is preferred, placed on ipsilateral side of Pneumothorax
- Avoid Subclavian Central Line (unless on same side as the Pneumothorax)
-
Coagulopathy (increased bleeding risk such as Hemophilia, Thrombocytopenia)
- Internal Jugular Central Line is preferred
- Avoid Subclavian Central Line as it is a noncompressible site
-
Hypercoagulable state (increased thrombosis risk)
- Subclavian Central Line is preferred
- Avoid Internal Jugular Central Line (highest risk site for DVT)
VIII. Approach: Site Selection by circumstance
- Crashing patient (Code, CPR) or Trauma patient (C-Spine Immobilization)
- Intraosseous Access
- Femoral Line
- Replace with supraclavicular line (IJ, EJ, Subclavian) when stabilized
- Children
- Femoral Line (if intraosseous fails)
-
Central Venous Pressure monitoring or Sepsis catheter
- Supraclavicular line (IJ, EJ, Subclavian)
IX. Approach: Pediatric Patients
- Central catheter sizes in children
- Infant: 3 French (24 gauge)
- Toddler/Preschool: 4 French (20 gauge)
- School age: 5 French (18 gauge)
- Catheter placement pearls
- Sedation allows for procedure (e.g. Ketamine 4 mg/kg IM)
- May use introducer (catheter over needle only) for initial Resuscitation
- May later, use guidewire through introducer catheter to place standard Central Line
- Catheter wire kinking, looping or fracturing (or dilator displacement)
- Gently move the wire in and out of dilator while dilator is being advanced
- Dilator misdirected down divergent path
- Rotate the dilator while inserting through subcutaneous tissue
- References
- Claudius, Behar, Chang and Santillanes in Herbert (2016) EM:Rap 16(4): 3-4
- Claudius, Behar and Hofmann, Santillanes, Bowman in Herbert (1018) EM:Rap 18(6):13-4
X. Approach: Securing Central Line and Maintenance
- Line holders
- Apply the white (inner) and blue (outer) line clips at 2 cm from the skin entry site
- One hole for Suture on each side of the clamp
- Apply the antimicrobial, bio-patch under the line at the skin entry site (with blue side of patch up)
- Proximal attachment (at base of the triple lumens)
- One hole for Suture on each side
- Suture the line in place
- Anesthetize the skin at each of the four Suture holes
- Use a 2-0 Silk Suture with curved needle (typically not in the Central Line kit) and needle driver
- Apply a sterile, transparent Occlusive Dressing over the Central Line entry
- Skin entry site and bio-patch should be clearly in view
- Triple lumen ports will exit at the notch in the Occlusive Dressing
- A second Occlusive Dressing with wings is applied beneath the ports to further secure line
- Apply the white (inner) and blue (outer) line clips at 2 cm from the skin entry site
- Mark the entry
- Using a marker on the Occlusive Dressing, write the date, time and provider initials
- Maintenance
- Check Central Lines daily for signs of infection
- Change Central Lines at 10 days or at signs of infection
- Consider Central Line removal when not used for >1 day
XI. Preparations: Devices
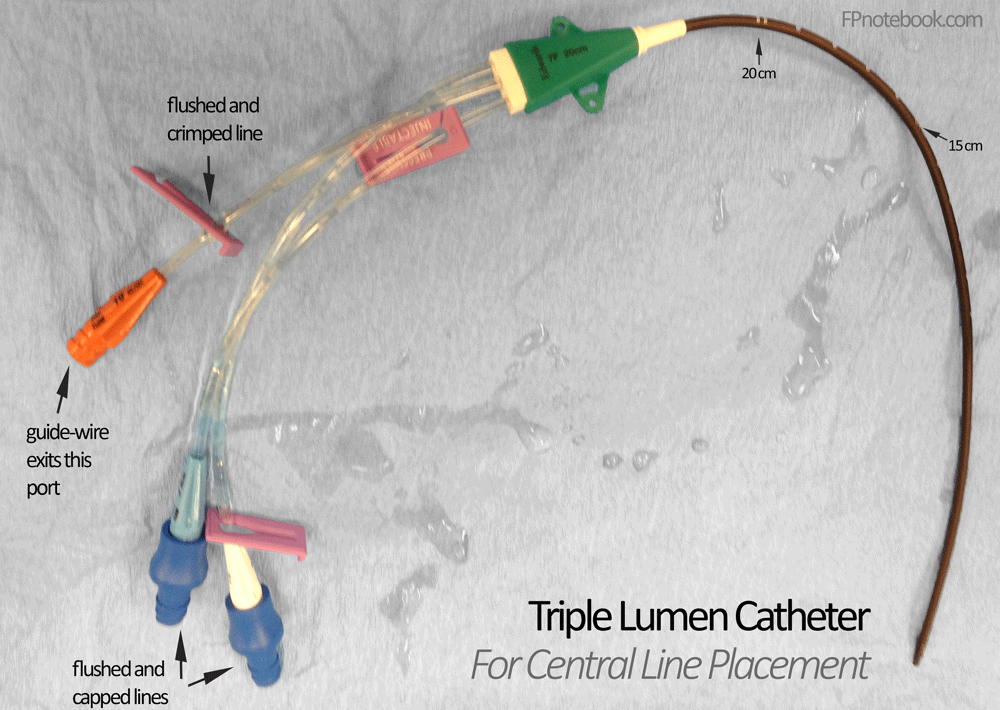
- Triple lumen catheter (typical Central Line)
- Double lumen catheter
- Hemodialysis catheter
- Cordis catheter
- Indicated for Hemodialysis or critically ill patients requiring advanced hemodynamic monitoring
XII. Complications: General
- Catheter Related Bloodstream Infections (CRBI)
- Collateral injury to surrounding structures
- Pneumothorax (IJ, EJ, Subclavian Line)
- Bladder or retroperitoneal injury (Femoral Line)
- Immobilization-related effects
- Deep Vein Thrombosis (especially Femoral Line)
- Other cardiovascular-related effects
- Air Embolus
- Pre-flush all catheters with saline
- Perform in trendelenburg position (both CVC Placement and removal)
- Perform needle entry during patient expiration
- Ensure adequate patient hydration
- Hold thumb over introducer needle while readying to insert guidewire
- Confirm that all catheter ports are clamped or capped
- Syringe handles should be upright (bubbles rise away from syringe tip)
- Cardiac Dysrhythmia (esp. Atrial Fibrillation; VT may occur)
- Normalize Electrolytes if possible before CVC Placement (esp. Potassium and Magnesium)
- Observe patient on cardiac monitor during line placement
- Limit guidewire insertion to no more than 20 cm
- If Arrhythmia occurs, promptly withdraw guidewire to safe distance (out of atrium)
- Air Embolus
- Retained Central Catheter Guidewire
- Unrecognized at time of procedure in up to one third of cases
- Missed on post-procedure imaging while focused on other features (e.g. IV position, excluding Pneumothorax)
- Unrecognized in some cases for up to years after procedure
- Delayed diagnosis risks serious complications
- Dysrhythmias
- Cardiovascular injury
- Venous Thrombosis
- Cardiac Tamponade
- Death
- Removal
- Typically requires Intervention Radiology for wire retrieval under fluoroscopy
- If guide wire is still partially encased in IV catheter, negative pressure technique may be attempted
- Repeatedly aspirate from catheter to attempt drawing wire back into channel toward skin surface
- When wire reaches skin level, a clamp may be applied to catheter (and wire within), and both withdrawn
- References
- Broder (2023) Crit Dec Emerg Med 37(10): 18-20
- Unrecognized at time of procedure in up to one third of cases
- Central Line Occlusion
- Attempt to flush the line with saline first
- Alteplase (tPA) protocol
- Reconstitute 2 mg vial of Alteplase in 2 ml Normal Saline
- Instill 2 ml Alteplase solution into clotted port
- Wait 30 minutes, then attempt to aspirate blood
- If no blood aspirated, wait another 90 minutes and attempt aspiration again
- If still no blood aspirated after first tPA instillation
- Repeat instillation of another 2 ml Alteplase
- Reattempt aspiration at 30 and 90 minutes as above
- If able to aspirate blood
- Aspirate 5-10 ml blood and discard
- Irrigate catheter with multiple Normal Saline flushes
- References
XIII. Complications: Site Specific Risks (may direct site selection)
- Precautions related to Complication Rates
- Overall CVC Complications have decreased significantly in the last 20 years
- Site specific complications have also decreased significantly
- Reduced complication rates are largely related to mitigating risks
-
Internal Jugular Central Line
-
Deep Vein Thrombosis (DVT)
- As of 2020, all Central Lines (IJ, femoral and subclavian) all have similar DVT Risk (3-3.5 per 1000 catheter days)
- Previously >2 fold increased risk over Subclavian Central Line
- Timsit (1998) Chest 114: 207-13 [PubMed]
- Parienti (2015) N Engl J Med 373(13):1220-9 [PubMed]
- Infection risk (CLABSI)
-
Deep Vein Thrombosis (DVT)
- External Jugular Central Line
- Failed placement
- Pneumothorax
-
Subclavian Central Line
-
Pneumothorax (highest risk site)
- Pneumothorax risk was 1-3% in 2002 (and similar risk in 2020)
- Noncompressible (uncontrolled bleeding risk)
- Infection risk (CLABSI)
-
Deep Vein Thrombosis (DVT)
- As of 2020, all Central Lines (IJ, femoral and subclavian) all have similar DVT Risk (3-3.5 per 1000 catheter days)
-
Pneumothorax (highest risk site)
-
Femoral Central Line
- Deep Vein Thrombosis (DVT)
- Infection risk (CLABSI)
-
Arterial Puncture
- Risk 6-7% in 2002 (contrast with 3% for IJ and 0.5% for subclavian vein)
- Children
- Preferred site in children (lower risk than IJ)
- Overall Complications
- Femoral Lines now had similar risks to internal jugular: infection rate (1.2%), thrombus rate (1.4%)
- Femoral also had the lowest failed placement rate (5%) compared with 9% IJ and 15% subclavian
- Parienti (2015) N Engl J Med 373(13):1220-9 [PubMed]
- Reduced CVC duration (2-6 days) has significantly reduced complications
- Femoral Lines specifically have an average duration of 2.7 days
- Remove the Central Line as soon as Peripheral IV Access is suffiicient
- Casanegra (2011) J Hosp Med 6(1):33-6 +PMID: 20578050 [PubMed]
- Femoral Lines now had similar risks to internal jugular: infection rate (1.2%), thrombus rate (1.4%)
- References
XIV. Complications: Misplaced or Malpositioned Central Venous Catheter
- Background
- Central venous catheter (CVC) is considered malpositioned if its tip is not in the superior vena cava or right atrium
- Mild catheter tip migration is common, often with torso or neck movement
- More significant misplaced CVCs include catheter tip floated distally (e.g. from IJ into subclavian towards hand)
- Procedure: Arterial Misplacement
- Artery punctured with introducer needle (but not dilated)
- Artery dilated and catheter placed
- Leave in Place Pending Consultation
- Risk of Hemorrhage on large bore Arterial Line removal
- Consult vascular surgery or Intervention Radiology regarding guidance
- Procedure: Venous Misplacement - Catheter Repositioning or Replacement
- Prevention
- Right sided central veins are preferred (less likely for malposition)
- Guidewire should be inserted with its J-curve directed towards the heart at midline
- Catheter Repositioning
- Increases risk of infection and may be more difficult to redirect
- Perform under same sterile conditions as if placing a new catheter
- Requires determining length the catheter needs to be withdrawn before advancing again
- Thread a guidewire through catheter with its J-Curve directed medially toward heart
- Other measures
- Pull downward on ipsilateral arm
- Consider Balloon tipped 2F Fogarty Catheter (longer than CVC) to help float tip into correct position
- Compress the unintended vessel (e.g. subclavian vein) when attempting to reposition into SVC/atrium
- Catheter Replacement (preferred)
- Risks loss of access, but is preferred for decreased infection risk
- Practice same sterile technique and procedure as per new CVC Placement
- Double glove with 2 sets of sterile gloves
- Remove the first glove set after the old catheter has been removed
- New sterile catheter set reduces risk of infection
- Withdraw first catheter from malpositioned location, but still in vessel
- Thread a guidewire through catheter with its J-Curve directed medially toward heart
- Ideally, use a 60 cm guidewire (instead of a standard 45 cm guidewire)
- Alternatively guidewire from new set may be used to change over the old catheter
- Continue to thread the guidewire to proper distance (<20 cm)
- Ideally, use a 60 cm guidewire (instead of a standard 45 cm guidewire)
- Remove the old catheter
- Thread the new catheter over the guidewire
- Precautions
- Use portable XRay or Bedside Ultrasound to monitor catheter positioning during procedure
- Prevention
- References
- Warrington (2021) Crit Dec Emerg Med 35(4): 9
- Roldan (2015) West J Emerg Med 16(5): 658-64 +PMID: 26587087 [PubMed]
XV. Complications: Catheter Site Bleeding
- Apply manual pressure to bleeding site for 20 minutes (e.g. sandbag, compression device)
- Purse Stitch
- Woggle Technique
- https://cairweb.ca/en/news/a-pearl-i-learned-and-remembered-the-woggle-technique/
- https://www.stepwards.com/?page_id=24971
- Technique
- Suture (3-0 Monofilament) placed through skin, under the Central Line (careful not to puncture the line)
- Cut off the needle and pull the ends up, twist ends together and thread through an open stopcock
- Push the stopcock against skin (or against intervening gauze) and tighten the stopcock to cinch
- Leave in place for 30 minutes, release the stopcock and remove the Suture
- Sacchetti in Swadron (2022) EM:Rap 22(8): 8
- Other measures
XVI. Resources
- Internal Jugular Vein cannulation video (ACEP Critical Decisions Video)
- Subclavian vein cannulation from a supraclavicular approach video (ACEP Critical Decisions Video)
- Subclavian vein cannulation from an infraclavicular approach video (ACEP Critical Decisions Video)
- Femoral vein cannulation video (ACEP Critical Decisions Video)
XVII. References
- Killu and Sarani (2016) Fundamental Critical Care Support, p. 93-114
- Jacquet and Hong (2014) Crit Dec Emerg Med 28(5): 15-22
- Rutherford (2025) Anatomy of Central Venous Access, Hospital Procedures Course, attended 9/12/2025
- Swaminathan and Herbert in Majoewsky (2013) EM:Rap 13(9): 6