
II. Epidemiology
- Elderly (median age 70 years old)
- Those <65 years old with Multiple Myeloma represent only 15% of cases
-
Incidence: 36,000 new cases per year in United States (2025)
- Represents 1.8% of all new cancers in U.S.
- Deaths: 11,000 to 12,000 per year
III. Risk Factors
- Demographics
- Non-Hispanic black (RR 2, and associated highest mortality)
- Male gender
- Family History confers 2-4 fold increased risk (Autosomal Dominant trait)
- Associated conditions
- Associated exposures
- Methylene chloride
- Dioxin (agent orange)
- Associated with certain occupational exposures
IV. Pathophysiology
- Malignant proliferation of Plasma Cells
- Overproduce monoclonal Protein
- Results from various genetic alterations (e.g. translocations, somatic mutations)
- Plasmacytoma may also form solitary Plasma Cell Tumor
- Abnormal Immunoglobulin (IgG, IgM, IgA are most common)
- May also involve light chains (either kappa or lambda)
- On spectrum of plasma cell malignancy
- Spontaneous (de novo) onset in 80% of cases
- Less than a third of Multiple Myeloma patients have a preceding known history of MGUS or SMM
- Monoclonal Gammopathy of Undetermined Significance (MGUS) in 20% of cases
- Progression to Multiple Myeloma at rate of 1% per year (see MGUS for progression risks)
- Smoldering Multiple Myeloma (SMM)
- Progression to Multiple Myeloma at rate of 10% per year for first five years (then decreases)
- Clinical Multiple Myeloma
- Plasma Cell Leukemia (Plasmacytic Leukemia)
- Spontaneous (de novo) onset in 80% of cases
- Risk Factors for progression from MGUS or SMM to Multiple Myeloma (see below)
V. Symptoms
- Asymptomatic in 34% of cases (present with abnormal labs: Anemia, Proteinuria, Hypercalcemia)
- Back pain or bone pain (58%)
- Fatigue (32%)
- Pathologic Fracture (up to 34-40% of cases)
- Anorexia and weight loss (24%)
-
Paresthesias (5%)
- Wrist Pain (Carpal Tunnel related Neuropathy)
- Other presenting symptoms
VI. Signs: Bone Findings
- Osteolytic lesions
- Pathologic Fractures
- Palpable swellings on accessible bones
- Location
- Sternum
- Skull
- Ribs
- Vertebrae (May result in Spinal Cord Compression)
VII. Differential Diagnosis: General
- Primary or metastatic cancer
- Benign bone lesions
- Infections (Osteomyelitis, Vertebral Osteomyelitis)
- Hyperparathyroidism
- Vertebral Compression Fracture (Osteoporosis)
VIII. Differential Diagnosis: Plasma Cell Peripheral Disorder
- See Plasma Cell Peripheral Disorder
- Common
- Uncommon
- Waldenstrom Macroglobulinemia
- Amyloidosis
- B-Cell Non-Hodgkin Lymphoma
- Rare
- Plasmacytoma
- Plasma Cell Leukemia
IX. Labs: Initial
- Comprehensive Metabolic Panel (including Serum Calcium, Serum Albumin and Protein, Renal Function tests, Electrolytes)
- Hypercalcemia
- Serum Calcium >10.1 mg/dl (present in 28%, Serum Calcium >11 mg/dl in 13% of patients)
- Renal Insufficiency
- Serum Creatinine >1.3 mg/dl (present in 48%, Creatinine >2 mg/dl in 23% of patients)
- Hypercalcemia
-
Complete Blood Count with Platelets
- Normochromic Normocytic Anemia
- Hemoglobin <12 grams/dl (present in 65-73% of patients)
- Anemia is nearly always present at one point for every patient
- Normochromic Normocytic Anemia
- Other initial tests to consider
- Thyroid Stimulating Hormone (TSH)
- Acute phase reactants (ESR, C-RP)
- Serum Vitamin B12
- Urinalysis
- Proteinuria (bence jones Proteins)
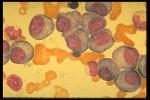
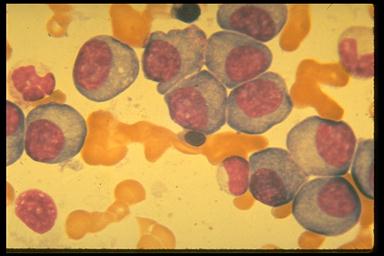
- Peripheral Smear
- Myeloma Cells
- Rouleaux of Red Blood Cells
X. Labs: Confirmatory
- Serum Protein Electrophoresis and Urine Protein electrophoresis for Monoclonal Peak
- Immunofixation electrophoresis of serum and urine
- Serum free light chain assay
- Serum quantitative Immunoglobulins
- 24 Hour Urine Protein
- Beta-2 microglobulin
- Lactate Dehydrogenase (LDH)
XI. Labs: Diagnosis - typically done in oncology
-
Bone Marrow Biopsy and aspirate (with cytogenetics, FISH, immunohistochemistry)
- Typically performed by oncology
XII. Imaging
-
Skeletal Survey (including Skull XRay)
- Recommended imaging for primary providers
- Classic "punched out" lytic lesions (66% of patients)
- Pathologic Fractures (26% of patients)
- PET/CT or whole body MRI
- Typically obtained in oncology
-
Bone Densitometry or DEXA (consider)
- Osteoporosis (23% of patients)
XIII. Diagnosis: Smoldering Multiple Myeloma
- Absence of Myeloma defining events (CRAB factors) AND
- No Amyloidosis AND
- Serum monoclonal Protein (IgG or IgA) >= 3 g/dl
- OR urinary monoclonal Protein >500 mg/24 hours
- OR Clonal Bone Marrow plasma cells 10 to 60%
XIV. Diagnosis: Multiple Myeloma
- Clonal Bone Marrow plasma cells >10% or biopsy proven bony or extramedullary Plasmacytoma AND
- Myeloma defining event (>=1 CRAB factors, absence suggests Smoldering Multiple Myeloma)
- Hypercalcemia
- Serum Calcium >11 mg/dl (or >1 mg/dl above upper range of normal)
- Renal Insufficiency
- Serum Creatinine >2 mg/dl (or GFR <40 ml/min)
- Anemia
- Hemoglobin <10 g/dl (or more than 2 g/dl below the lower limit of normal)
- Osteolytic Bone lesions
- Osteolytic lesions (one or more) on XRay, CT or PET/CT
- Other additional qualifying factors
- More than 1 MRI focal lesion >5 mm OR
- Clonal Bone Marrow plasma cells >60% OR
- Ratio involved to uninvolved serum free light chain >=100
- AND Involved free light chain >100 mg/L
- Hypercalcemia
XV. Diagnosis: Plasma Cell Leukemia
- All multiple meyloma criteria met AND
- Plasma cells >5% on conventional Peripheral Blood Smear white cell differential count
XVI. Staging
- Systems
- International Staging (ISS)
- Standard staging system was used most commonly (as of 2017)
- Revised International Staging (R-ISS)
- Better predictor of progression and survival than ISS (which it will likely replace)
- Durie-Salmon Staging
- International Staging (ISS)
- Stage I
- International Staging (ISS)
- Serum B2 Microglobulin <3.5 mg/L AND
- Serum Albumin >= 3.5 g/dl
- Revised International Staging (R-ISS)
- ISS Stage I AND
- Normal serum Lactate Dehydrogenase (LDH)
- No high risk Chromosomes on cytogenetic studies (e.g. del(17p), t(4;14), t(14:16))
- Durie-Salmon Staging
- Hemoglobin >10 g/dl
- Serum Calcium <12 mg/dl
- No bone disease or Plasmacytoma
- Serum paraprotein <5g/dl (IgG) or <3 g/dl (IgA)
- Urinary light chain excretion <4 g per 24 hours
- International Staging (ISS)
- Stage 2
- International Staging
- Serum B2 Microglobulin 3.5 to 5.5 mg/L
- Revised International Staging (R-ISS)
- Not R-ISS stage I or III
- Durie-Salmon Staging
- Not DSS stage I or III
- International Staging
- Stage 3
- International Staging
- Serum B2 Microglobulin >=5.5 mg/L
- Revised International Staging (R-ISS)
- ISS Stage III AND
- Increased Lactate Dehydrogenase (LDH) OR
- High risk Chromosomes (e.g. del(17p), t(4;14), t(14:16))
- Durie-Salmon Staging
- Hemoglobin <8.5 g/dl
- Serum Calcium >12 mg/dl
- Skeletal Survey with >2 lytic lesions
- Serum paraprotein >7 g/dl (IgG) or >5 g/dl (IgA)
- Urinary light chain excretion >12 g per 24 hours
- International Staging
XVII. Evaluation: IMWG Mayo 2/20/20 Rule for Smoldering Multiple Myeloma (SMM) Progression
- See Monoclonal Gammopathy of Undetermined Significance for MGUS related progression risk factors
- Criteria (score 1 point for each positive criteria)
- Serum monoclonal Protein >2 g/dl
- Ratio involved to uninvolved free light chain >20
- Marrow Plasma Cell Infiltration >20%
- Three Factor Interpretation: SMM Progression Risk in 2 years
- Score 0: Low Risk (6% risk of progression in 2 years)
- Score 1: Intermediate Risk (17% risk of progression in 2 years)
- Score 2-3: High Risk (44% risk of progression in 2 years)
- Four Factor Interpretation: SMM Progression Risk in 2 years
- Uses above three factor criteria and one additional point for any of the following chromosomal risks
- t(4;14)
- t(14:16)
- +1q
- Del13Q/Monosomy 13
- Score 0: Low Risk (6% risk of progression in 2 years)
- Score 1: Low-Intermediate Risk (23% risk of progression in 2 years)
- Score 2: Intermediate Risk (46% risk of progression in 2 years)
- Score 3-4: High Risk (63% risk of progression in 2 years)
- Uses above three factor criteria and one additional point for any of the following chromosomal risks
- References
XVIII. Management: Combination Therapy
- See oncology references for current management protocols
- Indication
- Symptomatic Multiple Myeloma
- Preparation
- Screen for HIV, Hepatitis B and Hepatitis C before initiating treatment
- Consider Antiviral and Antibiotic prophylaxis during treatment
- Protocol 1: Otherwise physically healthy patients (previously limited to age <65 years)
- First: High dose myeloablative Chemotherapy
- Four drug regimens (preferred in 2025 NCCN guidelines)
- Daratumumab (Darzalex, DRd) or Isatuximab (Sarclisa) AND
- Lenalidomide AND
- Bortezomib (VRd) AND
- Dexamethasone
- Older three drug regimen options
- CDT: Cyclophosphamide AND Thalidomide AND Dexamethasone OR
- VCd: Bortezomib AND Cyclophosphamide AND Dexamethasone
- Four drug regimens (preferred in 2025 NCCN guidelines)
- Next: Stem Cell Transplant (follows initial myeloablative Chemotherapy for 3 to 6 months)
- Autologous Stem Cell Transplant (ASCT) with high dose Melphalan
- Next: Maintenance Therapy
- One to 2 drug protocols taken for months to years (or indefinately) following Stem Cell Transplant
- First: High dose myeloablative Chemotherapy
- Protocol 2: Serious comorbidity (unable to tolerate marrow ablation and ASCT)
- Thalidomide AND Alkylating Agent (Melphalan, Cyclophosphamide or Chlorambucil) AND Prednisolone OR
- Bortezomib AND Doxorubicin AND Dexamethasone OR
- Bortezomib AND Thalidomide AND Dexamethasone (VTd)
- Medications used in first treatment of Multiple Myeloma
- Immunomodulating Agents
- Proteasome Inhibitors
- Monoclonal Antibodies
- Daratumumab (Darzalex, DRd)
- Elotuzumab (Empliciti)
- Isatuximab (Sarclisa)
- Alkylating Agents
- Corticosteroids (Dexamethasone)
- Administered concurrently with Chemotherapy to reduce light chain renal load (Kidney injury risk)
- Medications used to treat relapse
- Efficacy
- Stem Cell Transplant (ASCT) has increased median overall survival rate >10 years
- Palliative (Not curative)
- Relapse is common
XIX. Management: Adjunctive
-
Radiotherapy
- Localized conditions (e.g. severe bone pain, pathologic Fractures, local tumors)
- Pain management
- Analgesics
- Neuropathy medications
- Physical Activity
- Radiotherapy (localized severe bone pain)
-
Bisphosphonates
- Indicated in all treated patients (regardless of bony lesions)
- Treat for at least 2 years
- Preferred: IV Zoledronic acid or Pamidronate
- Alternative: Denosumab
- Additional
- Vitamin D Supplementation should also be given, and consider Calcium Supplementation with caution
- References
-
Venous Thromboembolism prophylaxis
- Reduces VTE Risk from 12-26% to 5-8% in Multiple Myeloma
- Indications
- Active treatment of Multiple Myeloma (esp. immunomodulatory agents)
- Continue for first 4-6 months after diagnosis (or until disease controlled)
- High risk patient prophylaxis
- Low Molecular Weight Heparin (e.g. Lovenox) 40 mg SQ daily
- Warfarin (Coumadin) and target INR 2-3
- Apixaban (Eliquis) 2.5 mg twice daily
- Rivaroxaban (Xarelto) 10 mg once daily
- Fondaparinux 2.5 mg once daily
- Low risk patient prophylaxis
- Aspirin 81 to 324 mg once daily
- Resources
- Impede-VTE score predicts VTE Risk specific to Multiple Myeloma
- References
- Prophylactic Antibiotics
- First 3 months of treatment (some cases)
- Trimethoprim-sulfamethoxazole (Septra, Bactrim) OR
- Fluoroquinolone
- Recurrent pneumococcal infections
- Proteasome Inhibitor therapy
- Antivirals (prevent Varicella Zoster Virus reactivation)
- Absolute Neutrophil Count <500/uL
- Other antimicrobial prophylaxis indications
- Viral seropositivity
- Multiple Myeloma new diagnosis
- Bispecific Antibody therapy (BsAbs)
- Chimeric Antigen Receptor T-Cell Therapy (CAR T-Cell Therapy)
- Autologous Stem Cell Transplant (ASCT)
- First 3 months of treatment (some cases)
-
Immunizations
- Before Treatment (at least 2 weeks)
- Also update Immunizations for close contacts of the patient
- Pneumococcal Vaccine
- COVID Vaccine
- Influenza Vaccine
- Recombinant Zoster Vaccine
- Respiratory Syncytial Virus Vaccine (if >=60 years old)
- After Autologous Stem Cell Transplant (ASCT)
- Give 50-70 days after
- Recombinant Zoster Vaccine
- Give 3 to 6 months after
- Pneumococcal Vaccine
- Also give after CAR T-Cell Therapy, BsAbs
- Pneumococcal Vaccine
- Give 6 months after
- Influenza Vaccine
- COVID Vaccine
- Give 6-12 months after
- Give 50-70 days after
- Before Treatment (at least 2 weeks)
XX. Management: Monitoring
- Symptomatic improvement
- Complication monitoring (see below)
- Weight loss
- Fatigue
- Bone pain
- Peripheral Neuropathy
- Venous Thromboembolism
- Infection
- Chemotherapy adverse effects and toxicity (e.g. Pancytopenia)
- Multiple Myeloma
- Decrease in M Component
-
MGUS and SMM monitoring
- Scheduled monitoring of paraproteins and serum light chains
- MGUS follow-up every 6 months (indefinitely)
- Smoldering Multiple Myeloma (SMM) follow-up every 3-6 months
- Monitoring for relapse or progression
- New or growing bone lesions (or Plasmacytoma)
- Hypercalcemia
- Hemoglobin decrease > 2 g/dl from baseline
- Serum Creatinine increase >2 mg/dl
- Hyperviscosity Syndrome
- High risk patient monitoring
- Labs every 3 months
- Complete Blood Count
- Serum Creatinine
- Serum Calcium
- Serum free light chain assay
- Urine and Serum Protein Electrophoresis (SPEP, UPEP)
- Imaging every year
- Whole body MRI, Low dose CT or PET-CT
- Labs every 3 months
XXI. Complications
-
Peripheral Neuropathy
- Nerve infiltration by amyloid
-
Immune Suppression
- Infection presenting complaint in 25% of patients
- Infection is the leading cause of morbidity and mortality in Multiple Myeloma
- Start empiric Antibiotics for febrile illness
- See above for prophylactic Antimicrobial Agents during treatment
- See prevention below for Immunizations
-
Hypercalcemia
- Initial Management
- Ensure euvolemia (consider crystalloid infusion)
- Corticosteroids
- Additional management in Refractory Cases
- Bisphosphonates (esp. zoledronic acid, preferred) or Denosumab
- Furosemide
- Other measures
- Initial Management
-
Renal Failure
- Renal Impairment is present in >30% of patients at time of Multiple Myeloma diagnosis
- Dexamethasone is often given prophylactically with Chemotherapy to reduce light chain renal load
-
General measures
- Correct Electrolyte abnormalities
- Ensure euvolemia
- Avoid Nephrotoxins
- Consult nephrology as needed
-
Acute Kidney Injury
- Multifactorial (free light chains at proximal tubules, Hypercalcemia, Dehydration, nephrotoxicity)
- Treat Acute Kidney Injury with crystalloid (e.g. NS, at least 3 L/day)
- Severe renal disease
- Hemodialysis may be required in up to 2% of patients
-
Venous Thromboembolism
- Relative Risk is 9 fold higher than general population (esp. in first 6 months of diagnosis)
- Consider other VTE Risk factors (e.g. Obesity, prior VTE, indwelling venous catheter, medical comorbidity)
- Impede-VTE score predicts VTE Risk specific to Multiple Myeloma
- https://www.mdcalc.com/calc/10498/impede-vte
- Consider VTE Prophylaxis for patients at high risk (see above)
-
Anemia
- Results from Bone Marrow invasion
- Consider differential diagnosis for Anemia
- Often improves with Multiple Myeloma treatment
-
Anemia management
- Red Blood Cell Transfusion for Hemoglobin <7 g/dl
- Erythropoiesis-stimulating agents may be considered (risk of thrombosis)
- Invasive bone lesions (80-90%)
- Pathologic Fractures
- Bone pain
- Osteoporosis
- Hypercalcemia
-
Vertebral Fractures
- See Vertebral Fracture
- Intravenous Bisphosphonates (Pamidronate, Zoledronic acid)
- Continue indefinately
- Reduces fracture Incidence and pain
- Surgical Intervention: Percutaneous Vertebroplasty or Kyphoplasty
- Indicated in refractory cases
- Radiation Therapy
- Indicated for Spinal Cord Compression
-
Hyperviscosity Syndrome (uncommon to rare)
- Findings: Fatigue, Headache, Visual disturbance, Retinopathy
- Treat with Plasma Exchange, antimyeloma Chemotherapy
XXII. Prognosis
- Invariably fatal but relates to staging
- Stage I: 62 Month median survival
- Stage 3: 29 Month median survival
- Treated patients live asymptomatically for years
- Five year survival is 61% as of 2020 (previously was 45% in 2007, and 30% in 1990)
- Stem Cell Transplant (ASCT) has increased median overall survival rate >10 years
- Median overall survival approaches 8 years with other modern management (including monoclonal antibodies)
- Mortality from cause unrelated to Myeloma: 25%
XXIII. Resources
- Multiple Myeloma Research Web Server
XXIV. References
- Hughes (2026) Am Fam Physician 113(3): 244-53 [PubMed]
- Kyle (2002) N Engl J Med 346: 564-9 [PubMed]
- Kyle (2003) Mayo Clin Proc 78:21-33 [PubMed]
- Michels (2017) Am Fam Physician 95(6): 373-83 [PubMed]
- Nau (2008) Am Fam Physician 78(7): 853-9 [PubMed]
- Rajkumar (2005) Mayo Clin Proc 80:1371-82 [PubMed]
- Rajkumar (2024) Am J Hematol 99(9): 1802-24 [PubMed]