
II. Epidemiology
- Most common Entrapment Neuropathy of the arm
- Prevalence: 3% of U.S. general population
- Incidence: 3.8 per 1000 person-years (increasing with age)
- Women outnumber men affected by 3 fold
- Bilateral in 50% of cases
- Associated with workplace repetitive hand activities
- Hand Paresthesias occur in 30% of computer users
- Only 10% of these meet criteria for Carpal Tunnel
- Only 3.5% of these have abnormal EMGs
- Stevens (2001) Neurology 56:1568-70 [PubMed]
III. Pathophysiology
- Compression of Median Nerve
- Occurs between transverse carpal ligament and underlying Carpal Bones
- Median Nerve adjacent to 9 flexor tendons whose synovial lining may become inflamed and enlarged
- Sensory deficits predominate
- Motor Nerves are much less susceptible than Sensory Nerves to compression
IV. Risk Factors: General
- Repetitive motion of hand and wrist
- Most common cause, and typically work related
- More common if significant force applied or hand-operated vibratory tool
- Local wrist or Hand Trauma
- Many predisposing conditions (see below)
V. Risk Factors: Predisposing Medical Conditions
- Obesity
- Hypothyroidism
- Diabetes Mellitus
- Acromegaly
- Rheumatoid Arthritis
- Gouty Arthritis
- Lyme Disease
- Amyloidosis
- Multiple Myeloma
- Double-Crush Syndrome
-
Edematous condition
- Third trimester of Pregnancy
- Symptoms subside after delivery
- Congestive Heart Failure
- Renal Failure
- Third trimester of Pregnancy
- Aberrant or Anomalous Muscles in wrist
- Proximal lumbrical insertion
- Distal extension of flexor superficialis Muscle
- Persistent thrombosed median artery
- Abnormal palmaris longus tendon
- Ganglion Cyst
- Lipoma
VI. Symptoms
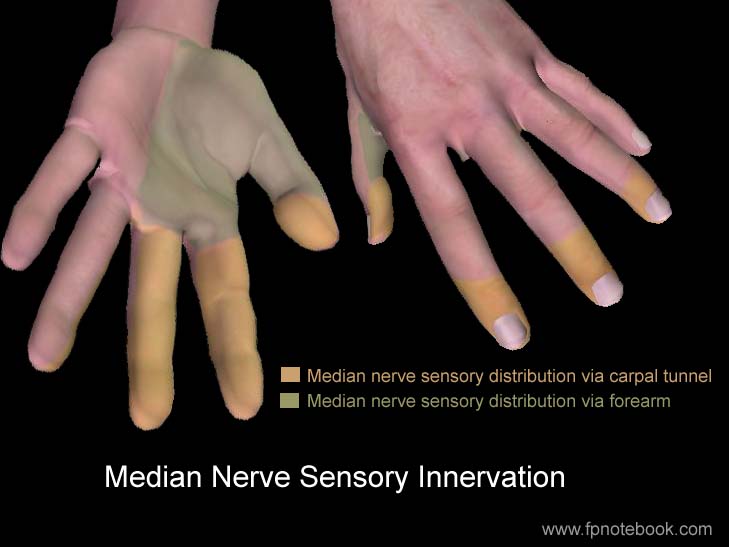
- Image: Median Nerve Sensory Innervation
- Pain and Paresthesias along Median Nerve course (palmar/volar surface)
- Electrical Sensation or Dysesthesias
- Radiation from the volar wrist into the thumb, index and middle finger
- Commonly involves only palmar/volar aspect of Index and Middle fingers
- May affect palmar aspect of all Median Nerve innervated 3.5 fingers (thumb to fourth finger)
- Radiation
- Proximal radiation into Forearm (may rarely radiate proximally into Shoulder and neck)
- May even present as Chest Pain (has resulted in ED Chest Pain cardiac work-ups)
- Radiation from the neck may occur with double crush injury (especially with bilateral involvement)
- Gradually increasing night pain (95% of patients)
- Increase in wrist swelling with inactivity
- Wrist flexion at night (may awaken patient)
- Numbness
- Describes "poor circulation" and "Stiffness"
- Despite which hand feels warm
- Weakness and Clumsiness of hand (severe cases)
- Decreased grip strength, with weak thumb abduction and opposition
- Timing
- Spontaneous onset
- Often interferes with sleep
- Provocative of Sensory and Motor Symptoms
- Repetitive wrist flexion or hand elevation
- Precipitated by Typing, holding phone, driving, painting, and wrist motion
- Palliative
- Shaking or moving hand
- Allow hand to hang down
- Flick Sign
- Flicking wrist as if shaking down Thermometer (often after night-time awakening)
- Test Sensitivity 93%, Test Specificity 96%
VII. Signs
- Precautions
- Observation
- Square-shaped wrist (depth dimensions approaches wrist width, esp in Obesity, OR 4.56)
- Modifying factors
- Pain not worse with resisted motion
- Flick Test (see above)
- Carpal Compression Test (64-90% sensitive, 83-90% specific)
- Direct pressure applied over the transverse carpal ligament for 30 seconds
- Positive for sensory symptoms within first 30 seconds
- Classic exam findings have individual poor predictive value (but combined 80% sensitivity, 92% Specificity)
- Tinel's Sign (44-70% sensitive, 94% specific, LR+ 1.3)
- Phalen's Maneuver (70-80% sensitive, 80% specific, LR+ 1.4)
- Hand elevation test
- Hands raised overhead for one minute
- Positive test if Median Neuropathy symptoms are reproduced in the first minute
- Differentiate from Thoracic Outlet Syndrome provoked with overhead arm (Elevated Arm Stress Test or EAST Test)
- Ahn (2001) Ann Plast Surg 46(2): 120-4 [PubMed]
- Tourniquet Test (not recommended as not sensitive and not specific)
- Inflate Blood Pressure Cuff on upper arm above systolic Blood Pressure
- Positive if Paresthesias and Numbness after inflation in first 60 seconds
- Sensory deficit over Median Nerve
- Sensory deficit predominates as Sensory Nerves are more susceptible to compression than Motor Nerves
- Hyperalgesia in classic Median Nerve distribution has high Likelihood Ratio
- Patient draws areas of pain or numbness on hand diagram
- Loss of Two Point Discrimination <=5 mm with caliper (33% Sensitive, 100% Specific)
- Resolution of pain with persistent numbness suggests permanent sensory loss
- DIP joint Sensation of the index and middle finger (anterior interosseous nerve) is often spared in Carpal Tunnel
- Motor deficits (late finding in severe Median Neuropathy)
- Weak thumb abduction and weakness
- Weak on grasping items, opening jars, buttoning clothing
- Thenar Muscle atrophy
- Associated with decreased grip strength
- Only present in severe, long-standing disease
- Other hand and wrist neuropathies will cause this as well
- Abductor pollicis brevis weakness
- Abduct thumb perpendicular to palm against examiner's resistance
- Weak thumb abduction and weakness
- Findings suggestive of alternative diagnosis
- Findings of Cervical Radiculopathy
- Wrist and hand with reduced range of motion (ROM should be unaffected in Carpal Tunnel)
- Thenar eminence with reduced Sensation
- Innervated by Median Nerve's palmar cutaneous branch (origin is proximal to Median Nerve)
- Suggests a Median Nerve injury in the neck or proximal arm
VIII. Diagnosis
-
Carpal Tunnel Syndrome Six Item Evaluation Tool (CTS-6 Evaluation Tool)
- Positive result (>=12, LR+ 4.5) is suffiicient evidence for diagnosis (without further diagnostics)
- Findings with highest predictive value
- Classic hand symptoms in median distribution
- Decreased Pain Sensation at index palmar surface
- Weak thumb abduction
- Thenar atrophy (99% Test Specificity)
- References
IX. Differential Diagnosis
- Tenosynovitis
- Flexor carpi radialis tenosynovitis
- Extends from proximal 1st Metacarpal to medial epicondyle
- De Quervain's Tenosynovitis
- Affects extensor pollicis brevis, abductor pollicis longus
- Flexor carpi radialis tenosynovitis
- Other Neuropathy
- Cervical Radiculopathy (C6 nerve)
- Median Nerve compression at elbow (Pronator Syndrome)
- Ulnar Tunnel (or Cubital Tunnel)
- Peripheral Neuropathy (e.g. Diabetes Mellitus)
-
Degenerative Joint Disease
- Wrist Osteoarthritis
- Thumb carpometacarpal Osteoarthritis
- Vascular conditions
- Raynaud Syndrome
- Vibration white finger (occurs with vibratory hand tools)
X. Imaging
-
Ultrasound
- See Median Nerve Measurement on Ultrasound
- Not needed for Carpal Tunnel diagnosis if CTS-6 Evaluation Tool is positive
- Highest efficacy when wrist Median Nerve cross sectional area is compared with Forearm measurement
- Noninvasive, painless test with high efficacy (for experienced operators) and evaluates other wrist structures
-
Wrist XRay (only if indicated)
- Consider Wrist XRay if bone or joint disorders are suspected
- Evaluate for local bony abnormality
- Other diagnostic studies (CT, MRI)
- Not typically indicated
- May consider Cervical Spine MRI if double crush injury is suspected (or suggested by Nerve Conduction Study)
XI. Diagnostics
-
Nerve Conduction Studies (Electromyography, EMG)
- Not needed for Carpal Tunnel diagnosis if CTS-6 Evaluation Tool is positive
- Indicated in severe Carpal Tunnel, unclear cases or in pre-surgical assessment of severity
- Delayed electrical conduction across wrist at the Median Nerve
- Axonal loss or Muscle denervation is an indication for surgery
- Efficacy: 56-85% sensitive, 94-99% specific
- Normal in up to one third of patients with mild Carpal Tunnel
XII. Grading: Severity
- Mild Carpal Tunnel
- Intermittent, occassional symptoms of pain and Paresthesias
- Moderate Carpal Tunnel
- Awakens with Carpal Tunnel pain frequently at night
- Activity provokes symptoms, but does not impair function
- No neurologic deficits on exam (motor or sensory)
- Severe Carpal Tunnel
- Thenar atrophy
- Weak thumb abduction or opposition
- Persistent sensory loss
XIII. Management: General Conservative Measures
- Precautions
- Severe Carpal Tunnel symptoms should prompt early EMG
- Early referral to surgery if EMG positive for axonal loss or Muscle denervation
- Efficacy
- Spontaneous resolution in non-severe CTS with Placebo, within 2 years: 50%
- Short-term: 80% respond
- Long-term: 80% of responders recur after one year
- Eliminate cause and modify work conditions
- Avoid repetitive Trauma (esp. high force, and with repeated hand gripping or pinching)
- Avoid the extremes of wrist flexion or extension
- Avoid vibratory tool use
- Employ ergonomics (wrist rest, adjust chair/desk, voice recognition software)
-
Wrist Splint or Wrist brace (neutral position)
- Polypropylene occupational Wrist Splint
- Maintains wrist in neutral position
- Do NOT use a hyperextension (dorsiflexion) brace which may exacerbate symptoms
- Modify the cock-up (hyperextension) brace by straightening the aluminum bar inside the brace
- Most effective if started early (within 3 months)
- Use the splint for at least 1 to 2 months (up to 6 months) at nighttime
- Wearing splint only during the night appears as effective as continuous use (day and night)
- Original studies had best benefit when worn during both day and night (continuously)
- Wrist and Hand Exercises
- Local or Systemic Corticosteroid
- Carpal Tunnel Steroid Injection (preferred)
- May repeat injection after 6 months
- Rare risk of Median Nerve injury, tendon rupture
- Improves symptoms and function for 3 to 6 months
- Less need for surgery (NNT 7) at one year
- Similar outcomes to night Splinting at 6 months (slightly better than Splinting at 6 weeks)
- Does not significantly reduce need for surgical intervention in the longterm (5 years)
- Ashworth (2023) Cochrane Database Syst Rev (2):CD015148 [PubMed]
- Chesterton (2018) Lancet 392(10156): 1423-33 [PubMed]
- Ly-Pen (2005) Arthritis Rheum 52:612-9 [PubMed]
- Consider Systemic Corticosteroids (NOT recommended)
- Less effective and more adverse effects than with local injection
- First: Prednisone 20 mg orally daily for 14 days
- Next: Prednisone 10 mg orally daily for 14 days
- Chang (1998) Neurology 51:390-3 [PubMed]
- Avoid ineffective injection strategies
- Platelet rich plasma injection is not effective
- Hydrodissection with prolotherapy is lacking evidence
- Carpal Tunnel Steroid Injection (preferred)
-
Analgesics: NSAIDs (e.g. Ibuprofen) or Acetaminophen
- Variable efficacy (unlikely to offer benefit beyond transient pain relief)
-
Pyridoxine may be indicated in pregnancy
- Dose: Pyridoxine 25-50 mg PO tid
- Unproven benefit
- Reference
XIV. Management: Physical Therapy or Hand Therapy
- Hand therapy conservative measures are effective (see above),
- Other specific therapies are NOT recommended and are NOT found to have longterm efficacy (or evidence)
- Avoid shock wave therapy, laser therapy, pulsed radiofrequency, massage therapy, kinesiology taping
- Local Therapeutic Ultrasound for 6 weeks may provide relief for up to 6 months
- Hand therapy Ultrasound and Carpal Bone mobilization have insufficient evidence
- Nerve glide Exercises are NOT recommended
- Described for historical reasons
- May theoretically untether a compressed Median Nerve
- However in practice, does not improve outcomes when added to Splinting
- Abdrolrazaghi (2023) Hand 18(2): 222-9 [PubMed]
- Technique (repeated each for 10-15 repetitions)
- Hyperextend hand against wall
- Wrist rotation against wall
- Repeat wrist rotation with neck lateral bending to either side
- Alternate finger extension with clenched fist
- Video Resource
XV. Management: Surgical Release Transverse Carpal Ligament
- Indications
- Early surgery for moderate to severe Median Nerve injury (by EMG)
- Persistent symptoms refractory to conservative therapy after 3-4 months
- Progressive or persistent motor weakness (grip strength) or thenar Muscle atrophy
- Efficacy
- General
- Results in prompt, permanent pain relief
- Very effective in 66% of patients (some studies report 70-90% of cases)
- May be effective even if EMG normal
- Longterm efficacy (>3 months after surgery)
- Mixed results in longterm studies of surgical versus non-surgical results
- Splinting and Corticosteroids injections may result in similar longterm outcomes to surgery
- Surgery may not lead to longterm significantly decreased symptoms or improved function
- Lusa (2024) Cochrane Database Syst Rev 1(1):CD001552 +PMID: 38189479 [PubMed]
- Open versus endoscopic repair
- Earlier return to work by 8 days with endoscopic repair
- Fewer complications (infection, scarring) with endoscopic repair
- Equivalent longterm outcomes with either endoscopic or open repair
- References
- General
- Course
- Sensory, Motor function improvement may take months
- Post-operative Splinting is NOT recommended
- Results in increased stiffness and does not improve outcomes
- Early mobilization results in better range of motion, strength and return to ADLs
- Postoperative rehabilitation is not typically recommended
- No evidence of benefit in outcomes
- Adverse affects
- No Disability from sectioning transverse ligament
- Residual discomfort may continue from tenosynovitis
- Complications (<2%)
- Median Nerve branch injury
- Hypertrophic, painful scar
- Superficial Palmar ArchLaceration
- Pillar pain adjacent to ligament release
- Incomplete transverse ligament division
- May result in refractory, persistent symptoms requiring repeat surgery (3% of patients)
XVI. References
- Alvarez (2024) Am Fam Physician 109(6): 571-2 [PubMed]
- D'Arcy (2000) JAMA 283(23): 3110-7 [PubMed]
- Katz (1994) Am Fam Physician 49(6):1371-9 [PubMed]
- Keith (2009) J Am Acad Orthop Surg 17(6): 389-96 [PubMed]
- Keith (2009) J Am Acad Orthop Surg 17(6): 397-405 [PubMed]
- LeBlanc (2011) Am Fam Physician 83(8): 952-8 [PubMed]
- Silver (2021) Am Fam Physician 103(5): 275-85 [PubMed]
- Shapiro (2025) J Am Acad Orthop Surg 33(7): e356-66 [PubMed]
- Viera (2003) Am Fam Physician 68(2):265-72 [PubMed]
- Wipperman (2016) Am Fam Physician 94(12): 993-9 [PubMed]
- Wipperman (2024) Am Fam Physician 110(1): 52-57 [PubMed]