
II. Indications
- Refractory Major Depression
- Anxiety Disorder
- Atypical Depression
- Refractory Depression
- Bulimia
- Social Phobia
- Narcolepsy
- Parkinsonism
- Multiple System Atrophy
III. Background
- Among the first Antidepressants developed (1950s)
IV. Precautions
- Limit use to refractory mental health or neurologic conditions due to high risk of adverse effects and Drug Interactions
- Tyramine-free diet must be followed
- Continue for two weeks after stopping medication
- See Tyramine Containing Foods
- Stop 2 weeks before starting another Antidepressant
- Taper Phenelzine (Nardil) slowly when stopping
- See Antidepressant Withdrawal
- Reduce dose by 15 mg/day every 2 weeks (or 10%/week)
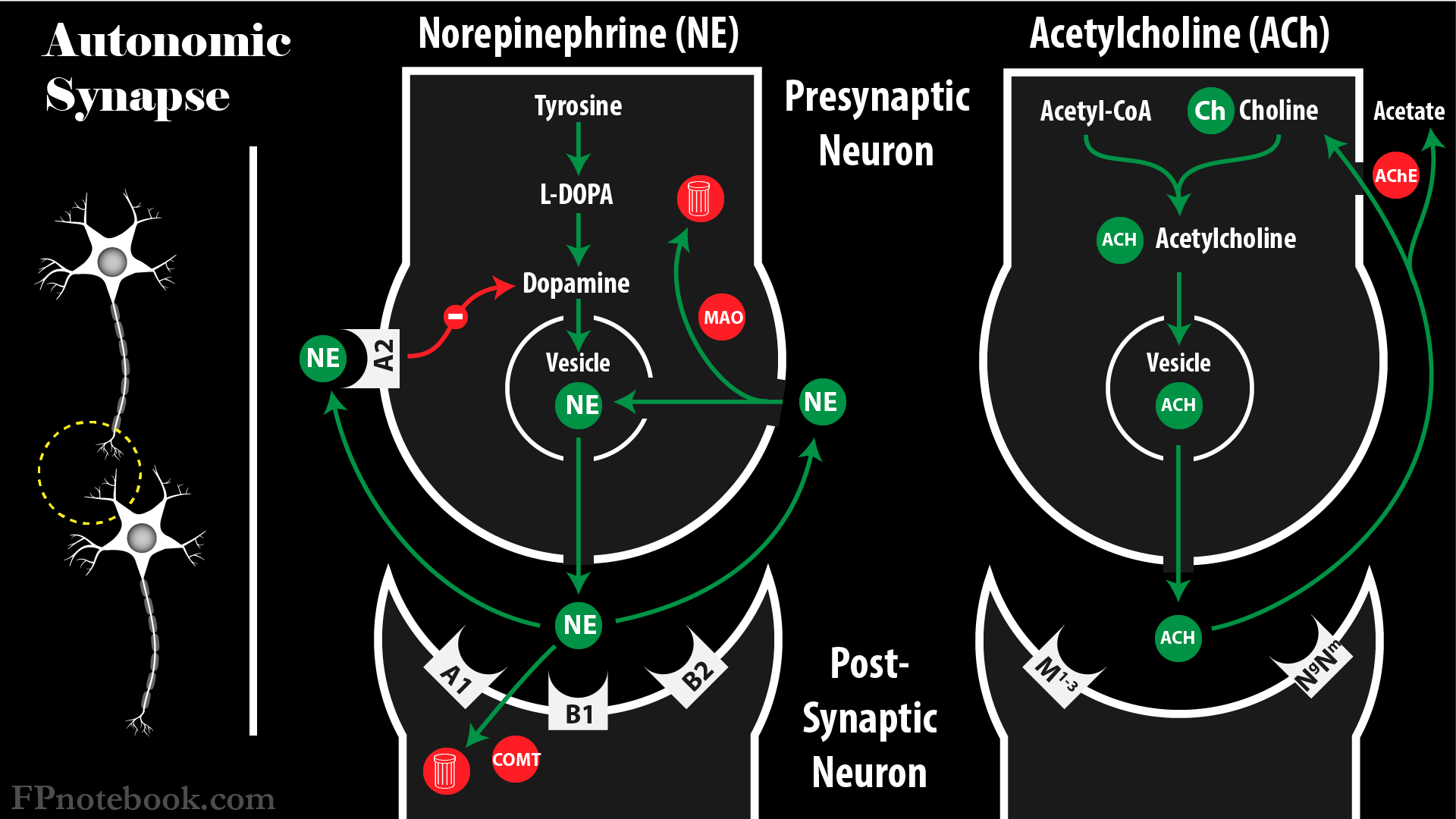
V. Mechanism
- Inhibits monoamine oxidase
- Monoamine Oxidase is the enzyme that breaks down biogenic amines (e.g. Norepinephrine, Serotonin, Dopamine, Tyramine)
- Type A Monoamine Oxidase affects Gastrointestinal System (intestinal tract, liver, placenta)
- Metabolizes Serotonin and Norepinephrine (as well as Dopamine, tyramine)
- Type B Monoamine Oxidase affects Central Nervous System (as well as liver and Platelets)
- Metabolizes phenylethylamine, methylhistamine and tryptamine (as well as Dopamine, tyramine)
- Type A Monoamine Oxidase affects Gastrointestinal System (intestinal tract, liver, placenta)
- Monoamine Oxidase is the enzyme that breaks down biogenic amines (e.g. Norepinephrine, Serotonin, Dopamine, Tyramine)
- Most MAO Inhibitors block MAO irreversibly for weeks (only Moclobemide and Safinamide are reversible)
- MAO Inhibitors have a similar structure to Amphetamine
- Older MAO Inhibitors are nonspecific and affect both Type A and B (e.g. trancypromine, Phenelzine)
- Selegiline is specific for Type B and is used in Parkinsonism
- MAO Inhibition increases synaptic concentration of monoamines
- Serotonin
- Norepinephrine
- Dopamine
- Tyramine
- Images
VI. Preparations: Non-Selective (Inhibit both MAO-A and MAO-B)
- Hydrazine (hepatotoxicity risk)
- Isocarboxazid (Marplan): No longer manufactured in U.S.
- Dosing: 10 mg PO bid
- Maximum: 60 mg per day
- Phenelzine (Nardil)
- Dosing: 15 mg PO tid
- Maximum: 90 mg per day
- Isocarboxazid (Marplan): No longer manufactured in U.S.
- Non-hydrazine
- Tranylcypromine (Parnate)
- Dosing: 10-40 mg/day in divided doses
- Maximum: 60 mg per day
- Tranylcypromine (Parnate)
VII. Preparations: Selective MAO Inhibitors
- Selective MAO-A Inhibitors
- Moclobemide (reversible MAO Inhibitor)
- Major Depression: 150 mg orally twice daily after meals
- Maximum dose: 600 mg/day (divided twice daily)
- Moclobemide (reversible MAO Inhibitor)
- Selective MAO-B Inhibitors (Parkinsonian agents)
- Selegiline (Eldepryl, Emsam)
- Major Depression: Transdermal patch 6 mg/24 hours (maximum dose 12 mg/24 hours)
- Parkinsonism: 5 mg orally twice daily at breakfast and lunch
- Rasagiline (Azilect)
- Parkinsonism: 0.5 mg orally daily (may be increased to 1 mg orally daily)
- Safinamide (Xadago, reversible MAO Inhibitor)
- Parkinsonism: 50 mg orally daily (may be increased to 100 mg orally daily after 2 weeks)
- Selegiline (Eldepryl, Emsam)
VIII. Preparations: Other agents with MAO Inhibitor Activity
- Linezolid
-
St John's Wort
- Contains Hypericin and Hyperforin (weak Type A and B MAO Inhibitors)
IX. Complications
-
Hypertensive Crisis (life-threatening)
- Occurs if tyramine or Sympathomimetic exposure
- Treat with Phentolamine (alpha-adrenergic Antagonist)
-
Overdose
- Hypotension to cardiovascular collapse
- Also presents with Serotonin Syndrome (Agitation, Hallucinations, hyperreflexia, fever, Seizures)
- Treat with Intravenous Fluids and direct acting Vasopressors (e.g. Norepinephrine)
-
Serotonin Syndrome
- Occurs with concurrent use of other Serotoninergic drug, or in Overdose
X. Drug Interactions
- MAO Inhibitors potentiate Sympathomimetics (Do not use with these medications within 2 weeks)
- Tyramine Containing Foods
- Sympathomimetics (Ephedra, Ephedrine, pseudophedrine, Phenylephrine)
- General Anesthesia
- Cyclobenzaprine (Flexeril)
- Specific Opioids
- Serotonergic Medications (Serotonin Syndrome risk)
XI. Metabolism
- MAO Inhibitors are inactivated by acetylation
- Slow acetylators (genetic predisposition) will have elevated serum levels of MAO Inhibitors
XII. Adverse Effects
- Anti-Histaminergic effects
- Dizziness
- Sedation
- Orthostatic Hypotension
- Weight gain
-
Dopaminergic effects
- Insomnia
- Myoclonal jerks
- Serotoninergic Effects
-
Anticholinergic Toxicity
- Dry Mouth
- Constipation
- Blurred Vision
- Urinary hesitancy
- Nausea
- Memory Dysfunction
- Other Effects
- Peripheral Edema
- Weakness
- Hepatotoxicity
XIII. References
- Sub Laban and Saadabadi (2022) Monoamine Oxidase Inhibitors, StatPearls, Treasure Island
- Nordt and Shoenberger in Herbert (2019) EM:Rap 19(3): 8-9
- Olson (2020) Clinical Pharmacology, Medmaster, Miami, p. 36-7