
II. Pathophysiology
- See Vomiting
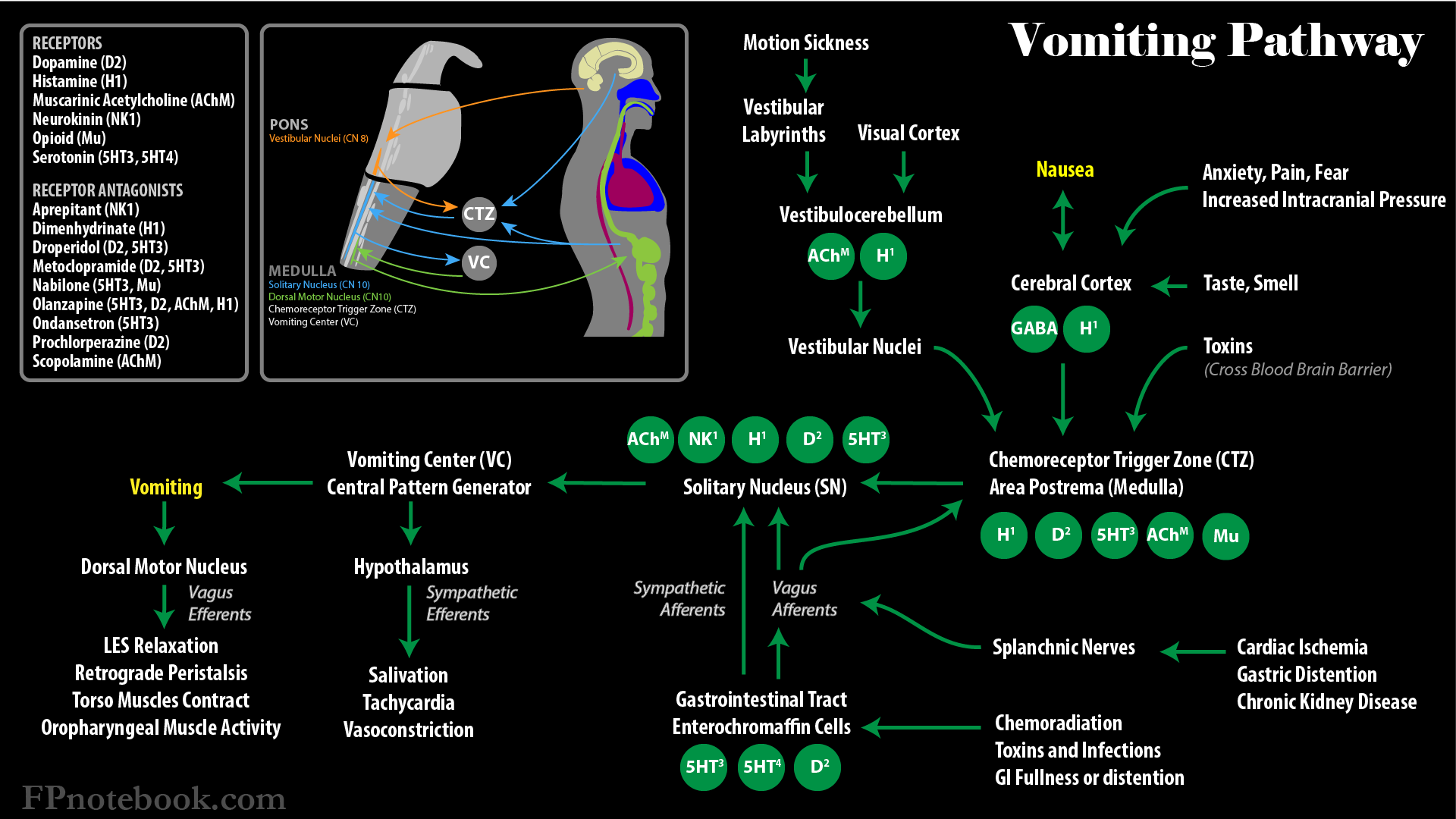
- Images
- Receptors involved in Nausea and Vomiting
- Serotonin (5-HT3, 5-HT-4) in GI, Neurologic and Chemical induced Vomiting
- Dopamine (D2) in GI and Chemical induced Vomiting
- Acetylcholine (ACh) in GI, Vestibular and Neurologic induced Vomiting
- Histamine (H1) in GI, Vestibular and Neurologic induced Vomiting
- Neurokinin (NK-1) in Neurologic and Chemical induced Vomiting
- GABA in anticipatory Nausea and anxiety
- Increased Intracranial Pressure with Neurologic induced Vomiting
III. Causes: General
- Common Causes
- Small Bowel Obstruction
- Autonomic failure
- Hypercalcemia
- Narcotic bowel Syndrome
- Disappears 2-3 weeks after starting Narcotic
- Associated with Intracranial Pressure
- Mnemonic: 11 M's
- Metastases (Cerebral, Liver)
- Meninges irritated (Increased Intracranial Pressure)
- Movement (Vestibular stimulation)
- Mentation (Anxiety)
- Medications (Opioids, Chemotherapy, NSAIDs)
- Mucosal irritation (NSAIDs, GERD, Hyperacidity)
- Mechanical obstruction (Constipation, Tumor, Cancer Related Bowel Obstruction)
- Motility (Ileus, Opioids)
- Metabolic (HypercalcemiaHyponatremia, Uremia)
- Microbes (Local infection, Sepsis)
- Myocardial dysfunction (ischemia, CHF)
IV. Causes: Chemotherapy
V. Approach: General Rules
- Attempt to identify a cause
- Consider combining Antiemetics if one not effective
- Use from different classes
- Avoid Nasogastric Tubes
VI. Management: General
- Always consider non-pharmacologic management first
- Small Frequent Meals
- Avoid bland foods (patient eats what they want)
- Starting Antiemetic agents
- Prochlorperazine (Compazine)
- Dimenhydrinate (Dramamine)
- Metoclopramide (Reglan)
- Consider specific agents
- Chemotherapy-Induced Vomiting (see below)
- Anxiety related Nausea: Benzodiazepines, Cannabinoids
- Bowel Obstruction: Octreotide
- Gastroparesis: Metoclopramide
- Increased Intracranial Pressure: Dexamethasone
- Opioid-related bowel dysfunction: Methylnaltrexone
- Refractory Nausea
- Combine 2-3 drugs from above
- Consider Haloperidol (Haldol)
- Start at 0.5 to 2 mg PO IV or SC q6 hours
- Titrate to 10 to 15 mg total daily dose
- Consider adding Prednisone or Dexamethasone
- Consider Cannabinoids
-
Emesis continues
- Consider Rectal route (e.g. Compazine)
- Consider Subcutaneous Route (e.g. Haldol)
- Consider Transdermal route (e.g. Scopolamine)
- Other cause specific management
- See Cancer Related Bowel Obstruction
- Anxiety: Benzodiazepines or Cannabinoids
- Gastroparesis: Metoclopramide (Reglan)
- Increased Intracranial Pressure: Dexamethasone
- Medication related
- See Chemotherapy related Nausea treatment as above
- See Opioid Adverse Effect Management for Opioid-Induced Nausea
- Other medication selection precautions
- Comorbid Delirium
- Dry Mouth (Xerostomia)
- Avoid orally disintegrating tablets (requires Saliva to dissolve tablet)
- Cardiac disease (e.g. CHF, CAD)
- Exercise caution with agents that prolong QTc
- Lung Disease (e.g. COPD, ILD) with Pleuritic Pain
- Consider Anxiolytics (e.g. Benzodiazepines) for Dyspnea-related Nausea
- Liver disease (e.g. end-stage Cirrhosis) with Ascites
- Consider Metoclopramide (Reglan) for prokinetic effects (e.g. associated Gastroparesis)
- Neurologic disease (e.g. ALS, Dementia, Parkinsonism, stroke)
- Caution in Dysphagia and aspiration risk
- If Tube Feedings are used, avoid large boluses
- In Parkinsonism, avoid anti-Dopaminergics (e.g. Haloperidol, Droperidol, Prochlorperazine, Metoclopramide)
VII. Management: Chemotherapy-Induced Vomiting
- Background
- Regimens are started before Chemotherapy and continued for 3 days after
- Typical dosing 30 minutes before Chemotherapy
- Ondansetron 16 to 32 mg IV or 24 mg orally (or other 5-HT3 Antagonist) AND
- Dexamethasone 4 mg (often 20 mg orally daily given)
- 5-HT3 Antagonists used in Chemotherapy induced Vomiting
-
Chemotherapy with the strongest emetic effects (e.g. Cisplatin)
- Ondansetron (or other 5-HT3 Antagonist) AND
- Dexamethasone AND
- Aprepitant (or Zyprexa)
- Akynzeo (Palonosetron and Netupitant) may be used as a single dose prior to Chemotherapy
- Akynzeo lasts for 3 days and can be used in place of Aprepitant and Ondansetron
-
Chemotherapy with the moderate emetic effects (e.g. Oxaliplatin)
- Ondansetron (or other 5-HT3 Antagonist) AND
- Dexamethasone
- Consider adding Aprepitant (or Zyprexa) if needed
-
Chemotherapy with the lower emetic effects (e.g. Paclitaxel)
- Dexamethasone (e.g. 20 mg orally) for a single dose prior to Chemotherapy
- Alternatives to Dexamethasone
- Delayed Chemotherapy-Induced Nausea
- Metoclopramide (Reglan) 1-2 mg IV or orally every 2-4 hours AND
- Dexamethasone 4 mg
- References
- (2014) Presc Lett 21(12): 71
VIII. Managemeny: Antiemetics
-
Anticholinergics
- Consider in excess oral secretions
- Scopolamine (Transdermal 1.5 mg patch) 1-2 patches replaced every 48 to 72 hours
-
Phenothiazines
- Prochlorperazine (Compazine) 5-10 mg PO or IV every 6-8 hours or 25 mg rectally every 12 hours
- Promethazine (Phenergan) 25-50 mg orally, rectally or IV every 6 hours
- Overused, sedating and relatively ineffective in Palliative Care
- Chlorpromazine (Thorazine) 12.5 to 25 mg IV every 6-8 hours or 25-50 mg orally every 8 hours
- Butyrophenones
- Haloperidol (Haldol) 0.5 to 2 mg orally or IV every 4-8 hours
- Droperidol (Inapsine) 1.25 to 2.5 mg IV
- Strong black box warning in U.S. due to risk of QT Prolongation, but appears safe
- Calver (2015) Ann Emerg Med 66(3): 230-8 +PMID:25890395 [PubMed]
- Thienobenzodiazepine
- Olanzapine (Zyprexa)
- Often dosed prophylactically at night (e.g. 2.5 mg ODT before bedtime)
- Olanzapine (Zyprexa)
-
Antihistamines
- Meclizine (Antivert)
- Indicated for vestibular associated Emesis
- Diphenhydramine (Benadryl) 12.5 to 50 mg orally, rectally, or IV every 4-12 hours
- Hydroxyzine (Atarax, Vistaril)
- Meclizine (Antivert)
- Gastrokinetic agents
- Consider in Gastroparesis, but avoid in suspected malignant Small Bowel Obstruction
- Metoclopramide (Reglan) 5-20 mg orally or IV every 6 hours
-
5-HT3 Receptor Antagonists
- Ondansetron (Zofran) 4-8 mg orally (esp. ODT dissolvable) or IV every 4-8 hours
- Granisetron (Kytril) 1 mg orally or IV twice daily
- Dolasetron (Anzemet)
-
Cannabinoids
- Consider in anticipatory Nausea
- Nabilone (Cesamet) 1-2 mg orally every 12 hours
- Dronabinol (Marinol) 5-10 mg orally, rectally or sublingual every 6-8 hours
-
Corticosteroids
- Consider in malignant Small Bowel Obstruction or Increased Intracranial Pressure
- Dexamethasone (Decadron) 2-8 mg orally or IV every 4-8 hours
- Benzodiazepines
IX. References
- (2003) Med Lett Drugs Ther 45(W1162B): 62-4 [PubMed]
- Albert (2017) Am Fam Physician 95(6): 356-61 [PubMed]
- Collis (2015) BMJ 351: h6249 [PubMed]
- Flake (2015) Am Fam Physician 91(5): 293-6 [PubMed]
- McGregor (2025) Am Fam Physician 112(5): 493-503 [PubMed]
- Ross (2001) Am Fam Physician 64(5):807-14 [PubMed]