
II. Epidemiology
- Bleeding Gums, Epistaxis and easy bruisability are common in healthy patients (occurs in up to 45%)
-
Menorrhagia is very common in women (5-10%)
- Bleeding Disorders contribute to up to 29% of Menorrhagia cases (esp. Von Willebrand Disorder)
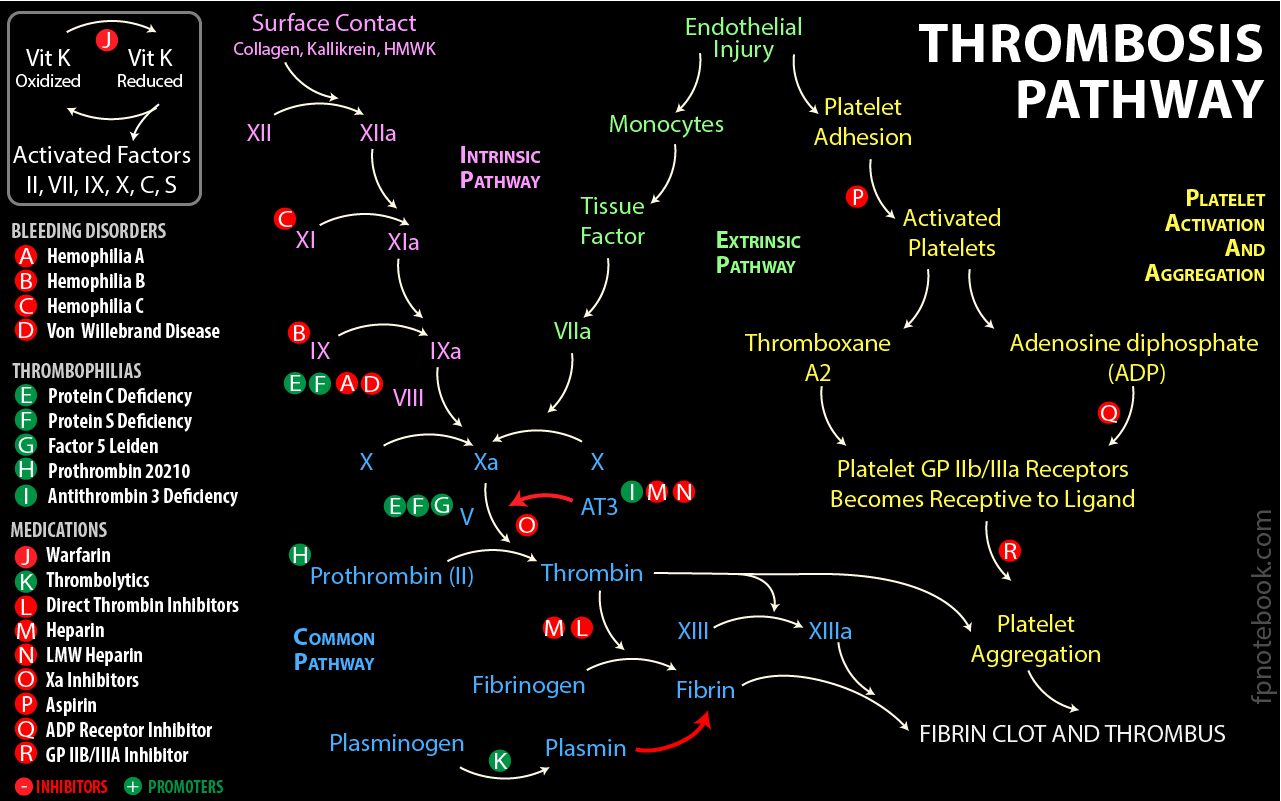
III. Pathophysiology
- See Clotting Pathway
IV. History: Bleeding or Bruising History
- Screening Questions for congenital Bleeding Disorder
- Bleeding or Bruising history
- Source of bleeding (e.g. skin Bruising, Epistaxis, GI Bleed)
- Severity of bleeding (e.g. degree of bleeding, size of Bruising)
- Duration of bleeding until controlled
- Triggers (e.g. Trauma, dental procedure, Vaginal Delivery)
- Menorrhagia history
- Spontaneous bleeding episodes
- Coagulation Disorders: Spontaneous hemarthroses (bloody joint effusions) and muscle Hematomas
- Platelet Disorders: Spontaneous mucocutaneous bleeding (e.g. Bleeding Gums, Epistaxis)
- Red flags suggestive of significant Bleeding Disorder
- Bleeding from >=2 mucocutaneous sites
- Epistaxis episodes >5 per year OR one episode lasting >10 minutes
- Bleeding duration >10 minutes after a minor Laceration
- Heavy and prolonged Menstrual Bleeding
- Unexplained Postpartum Hemorrhage
- Bleeding episodes >3 from a single site
- Bleeding episode requiring Blood Transfusion
V. History: Past Medical History
-
Family History of Bleeding Disorder (e.g. Hemophilia, Von Willebrand Disease)
- Include second-degree relatives, and back several generations
- Negative Family History does not exclude inherited Bleeding Disorder
- Medications and Substances
- Dietary history
- Restrictive diets may result in Vitamin C or Vitamin K Deficiency
VI. History: Symptoms or Clinical Clues
- Age of onset
- Young age
- Severe inherited Bleeding Disorders are typically diagnosed in the first few years of life
- Consider in excessive bleeding from Circumcision, umbilical stump, large or numerous Bruises
- All U.S. newborns are given IM Vitamin K (unless refused) to prevent Hemorrhagic Disease of the Newborn
- Teens
- Von Willebrand Disease diagnosis is often delayed until Menarche (teen girls)
- Older age
- Thinning of skin and subcutaneous tissue, and capillary weakening leads to Bruising in older adults
- Young age
- Critical Illness or hospitalization
- Acute Diarrhea (E. coli 0157:H7)
- Upper Respiratory Infection (esp. Streptococcal Pharyngitis)
- Chronic Bleeding Disorder
- Systemic Lupus Erythematosus
- Ehlers-Danlos Syndrome
- Hypermobile joints
- Von Willebrand Disease
- Menorrhagia (most common), recurrent Epistaxis or Gingival Bleeding
- Often delayed diagnosis with normal basic coagulation labs (until Platelet closure time is checked)
- Hemophilia A (Factor VIII) or Hemophilia B (Factor IX) deficiency
- Hemoarthrosis or other soft tissue bleeding in males
- Hereditary Hemorrhagic Telangiectasia (Osler-Weber-Rendu Syndrome)
- Telangiectasias involving lips, Tongue, skin, nose and GI Tract
- Immune Thrombocytopenic Purpura
- Especially children (often following viral syndrome such as EBV, VZV or CMV)
-
Night Sweats, fever and weight loss (B Symptoms)
- Hematologic Malignancy (Leukemia, Myelodyspastic syndrome, Lymphoma)
-
Malnutrition
- Alcoholic Liver Disease (Alcoholic Cirrhosis)
- Vitamin C Deficiency
- Vitamin K Deficiency (esp. infants <6 months who did NOT receive as newborn)
-
Bruising
- Physical Abuse
-
Purpura Simplex
- Women with Bruising on arms and upper thighs
- Senile Purpura
-
Coagulation Disorders
- Associated with spontaneous hemarthroses (bloody joint effusions) and muscle Hematomas
- Pregnancy
- HELLP Syndrome
- Severe Preeclampsia with Hemolysis, elevated liver enzymes and Low Platelet Count
- HELLP Syndrome
VII. History: Example Presentations
- Excessive Newborn umbilical stump bleeding
- Associated disorders include coagulation Protein deficits, Factor XIII deficiency
- Occult Intracranial Hemorrhage may be associated
- Male infant with swollen joints
- Common presentation in Hemophilia
- May be associated with forehead Cephalohematomas, excessive post-Circumcision bleeding
- Post-viral syndrome in a previously healthy child
- Associated with Immune Thrombocytopenic Purpura
- May present with Petechiae or oral Purpura
- Adolescent females with heavy Menorrhagia
- Common presentation in Von Willebrand Disease
- May be associated with recurrent Epistaxis, severe Iron Deficiency Anemia
VIII. Signs: Abnormal Bleeding (multiple sites)
- Nasopharynx
- Gastrointestinal
- Hematemesis
- Melana
- Gynecologic
- Musculoskeletal
- Muscle Hematomas
- Hemarthrosis
- Skin
- Dcoument size, number, and location of lesions (and consider images for medical record)
- Lesions
- Petechiae (<2 mm)
- Purpura (2 to 10 mm)
- Ecchymosis (>10 mm)
- Telangiectasias
- Red Flags suggestive of Bleeding Disorder
- Truncal Bruising
- Five or more Ecchymosis (>10 mm)
-
Trauma
- Excessive bleeding from minor wounds
- Excessive bleeding following surgery or dental procedures
- Intracerebral bleeding event
- Consider physical abuse
IX. Signs: Clinical Clues
- Spontaneous hemarthrosis, muscle Hemorrhage or retroperitoneal bleeding
- Congenital Bleeding Disorder
- Mucocutaneous bleeding (Petechiae, Epistaxis, Gingival Bleeding, GI Bleeding, GU Bleeding)
-
Hepatomegaly
- Liver disorder
- Splenomegaly
- Joint Hyperextensibility
X. Causes
- Coagulation Disorder
- Platelet Disorders
- Vascular Disorders
- See Blood Vessel Wall Bleeding Disorders
XI. Labs: Initial
- Complete Blood Count with Platelets
- Peripheral Blood Smear
- ProTime (PT) with INR
- Activated Partial Thromboplastin Time (aPTT)
- Fibrinogen
- Comprehensive metabolic panel (Liver Function Tests and Renal Function tests)
- Bleeding Time is NOT typically used due to lack of standardization
XII. Evaluation: Based on initial testing
- See ISTH Bleeding Assessment Tool (ISTH-BAT)
- Normal PT, PTT, and Platelet Count/morphology
- Obtain labs
- Von Willebrand Factor Antigen
- Von Willebrand Factor Activity (risocetin Cofactor activity)
- Factor VIII Level
- AVOID Platelet Function Closure Time (PFCT, Platelet Function Analyzer-100)
- No longer recommended due to False Negatives in less than severe cases of Von Willebrand
- Abnormal labs
- Von Willebrand Disease (additional testing can identify type)
- Normal labs
- Refer to hematology for additional evaluation of Platelet function disorder
- May require light transmission aggregometry
- Obtain labs
- Partial Thromboblastin Time (PTT) abnormality and Normal PT/INR (Intrinsic Clotting Pathway Abnormal)
- PTT corrects with a PTT Mixing Study (patient plasma mixed 1:1 with normal plasma)
- Obtain Factor VIII, Factor IX, and Factor XI assays
- Hemophilia A (Factor VIII Deficiency, 85% of Hemophilia cases)
- Hemophilia B (Factor IX Deficiency, 15% of Hemophilia cases)
- Hemophilia C (Factor XI Deficiency, rare)
- Consider Von Willebrand's testing if low Factor VIII
- Von Willebrand Disease alone does not affect PTT
- Von Willebrand Disease with Factor VIII:C deficiency results in a mild increase in PTT
- Obtain Factor VIII, Factor IX, and Factor XI assays
- PTT does not correct with a PTT Mixing Study (mixed with normal blood)
- Obtain Lupus Anticoagulant
- Obtain Factor VIII Inhibitor
- PTT corrects with a PTT Mixing Study (patient plasma mixed 1:1 with normal plasma)
-
ProTime (PT) or INR prolonged and Normal PTT (Extrinsic Clotting Pathway Abnormal) - uncommon
- PT/INR corrects with Vitamin K Supplementation
- Replace Vitamin K as needed
- Assess for Malnutrition and malabsorption causes of Vitamin K Deficiency
- PT/INR does not correct with Vitamin K Supplementation
- Obtain Factor VII assay
- Also consider liver disease, early Disseminated Intravascular Coagulation
- Confirm not taking a Vitamin K Antagonist (e.g. Warfarin)
- PT/INR corrects with Vitamin K Supplementation
- BOTH ProTime (PT/INR) and Partial Thromboplastin Time (PTT) Abnormal
- Causes
- Comorbid advanced liver disease (e.g. Cirrhosis)
- Disseminated Intravascular Coagulation (DIC)
- Anticoagulant use (e.g. Warfarin, Heparin, Direct Thrombin Inhibitors)
- Common Clotting Pathway Disorder
- Factor X Deficiency (may also occur in Amyloidosis)
- Factor V Deficiency
- Factor II Deficiency (Prothrombin)
- Factor I Deficiency (Fibrinogen Deficiency)
- Labs
- Liver Function Tests
- Fibrinogen level
- Coagulation Factor Assays
- Causes
-
Platelet abnormality
- See Platelet Bleeding Disorders
- See Drug Induced Platelet Dysfunction
- See Thrombocytopenia
- Peripheral Blood Smear for microscopic Platelet abnormalities
- Platelet function tests (specialty lab typically ordered by hematology)
- Light transmission aggregometry (or, if not available, then PFA 100)
- Avoid Bleeding Time (low sensitivity and lack of standardization)
- Images
XIII. Management
- Hemorrhage Management
- Manage Specific Conditions
- Consider Acquired Coagulopathy
- Cirrhosis (decrease of both coagulant and Anticoagulant factors)
- End Stage Renal Disease (Anemia, Platelet Dysfunction)
- Rattlesnake bite (Fibrinogen deficiency)
- Massive Transfusion (Dilutional Coagulopathy)
- Disseminated Intravascular Coagulation (DIC)
- Constant oozing of blood from inserted lines, drains and tubes
- Multiple sites of Hemorrhage including Gastrointestinal Bleeding
- Hematology Consultation indications
- Significant finding on testing
- Preoperative concern for Bleeding Disorder
- Prior history of excessive bleeding with invasive procedures
- Nondiagnostic results with high clinical suspicion
- Major or excessive bleeding with minor Trauma
XIV. References
- Ferdjallah (2024) Mayo Clinic Pediatric Days, attended lecture 1/16/2024
- Allen (2002) Pediatr Clin North Am 49: 1239-56 [PubMed]
- Ballas (2008) Am Fam Physician 77:1117-24 [PubMed]
- Hughes (2024) Am Fam Physician 110(5): 504-14 [PubMed]
- Jones (2024) Am Fam Physician 110(1): 58-64 [PubMed]
- Neutze (2016) Am Fam Physician 93(4): 279-86 [PubMed]