
II. Definitions
- Immune System
- Defense mechanism against both errant native cells and foreign organism or substance invasion
- Distinguishes self from non-self
- Eliminates foreign organisms and substances
- Responses include humoral immune response and the cell-mediated response
- Organs (Thymus, Spleen, Tonsils, Lymphatic System, hematopoetic system)
- Cells (Lymphocytes, Granulocytes, Monocytes, Macrophages)
- Molecules (antibodies, complement, Cytokines)
- Defense mechanism against both errant native cells and foreign organism or substance invasion
- Innate Immunity (Natural Immunity)
- Generalized, immediate immune response not reliant on prior exposure
- Predates the evolution of the more specific Immunity provided by antibodies and Lymphocytes
- Adaptive Immunity
- Organism specific Immunity that relies on prior "memory" of exposure
- Immune System evolved beyond the more primitive Innate Immunity
- Humoral Immunity (Antibody and B Cell response)
- Cell mediated Immunity (T Cell Response)
-
Phagocyte (and Phagosome, Phagocytosis)
- Immune cells (Neutrophils and Monocytes/Macrophages) are White Blood Cells that engulf pathogens and foreign material
- Phagosomes are the membrane engulfed pathogens
- Often combined with lysis by Lysozymes
-
Lysosome (and Lysozyme)
- Lysozyme-containing vacuoles produced in cellular golgi apparatus
- Lysomsomes fuse with Phagosomes, resulting in pathogen lysis (esp. Bacterial cell walls)
- Lysosomes, like Phagosomes, are found in Phagocytes (Macrophages and Neutrophils)
-
Opsonin (and Opsonization)
- Proteins (e.g. Antibody, complement, C-Reactive Protein) that bind a pathogen surface, targeting it for Phagocytosis
III. Types: Innate Immunity (Natural Immunity)
- Physical Barriers
- Skin
- Mucosa (e.g. respiratory and Gastrointestinal Tract)
- Cilia (e.g. respiratory)
- Inflammatory Response
- C-Reactive Protein
- Increases with inflammation and tissue injury
- Binds Bacterial surface and facilitates Phagocytosis (by Macrophages and Neutrophils)
- Prostaglandins and Leukotrienes
- Fatty Acids released from injured cells, as well as Mast Cells
- Promote inflammation (e.g. vascular permeability, Neutrophil chemotaxis, stimulate Nociceptors)
- Kinin peptides (kallidin and bradykinin)
- Short-lived inflammatory Proteins that increase vascular permeability and result in arteriolar dilitation
- Cytokines
- Cytokine types include Interleukin, Interferon, Tumor Necrosis Factor, Colony-Stimulating Factor, TGF-beta
- Glycoproteins act in inflammatory and immune response via cell to cell communication
- Released from cells in response to a trigger (e.g. Antigen binding) and bind and activate Target Cells
- C-Reactive Protein
- Secretion Contents
- Lysozyme (e.g. in tears, Saliva and in Neutrophils)
- Enzymatically degrades cell walls
- Acid destroys acid-labile organisms
- Sweat Lactic Acid
- Stomach Gastric Acid (Hydrochloric Acid)
- Lysozyme (e.g. in tears, Saliva and in Neutrophils)
-
Phagosomes (Phagocytosis)
- Phagocytes such as Neutrophils (PMNs) and Macrophages attract and engulf organisms (Phagocytosis)
- Phagocytes attract organisms which in turn activate Phagocytosis
- Phagosomes are later lysed via Lysosomes (as below)
-
Lysosomes
- Neutrophil's and Macrophage's (Phagocytes) golgi apparatus produce Lysosomes (vacuoles) that contain Lysozyme
- Lysosomes fuse with Phagosomes to produce phagolysosomes, degrading the engulfed organisms
- Lysosomes may also release their contents extracellularly to lyse larger targets too large to engulf
-
Spleen responds to blood borne pathogens
- Red Pulp
- Vascular Sinusoids at the end of arterioles
- Filter blood of Red Blood Cells and non-immunogenic foreign material
- White Pulp
- Collections of Macrophages, plasma cells, dentritic cells and Lymphocytes
- Red Pulp
-
Natural Killer Cells (NK cells)
- Lymphocytes providing protection against Intracellular Bacteria and viruses
- NK cells bind Major Histocompatibility Complex 1 (MHC-1)
- NK cell mechanisms of infected cell destruction
- Cytoplasmic granules
- Perforin
- Generates pores on cells targeted for destruction
- Granzyme
- Induces programmed cell death (apoptosis) on entry into Target Cells
- Perforin
- Cytokines
- Interferon-Gamma (IFN-g)
- Activates Macrophages for Phagocytosis
- Interferon-Gamma (IFN-g)
- Cytoplasmic granules
- Image: NKC Mediated Destruction of Infected Host Cells
-
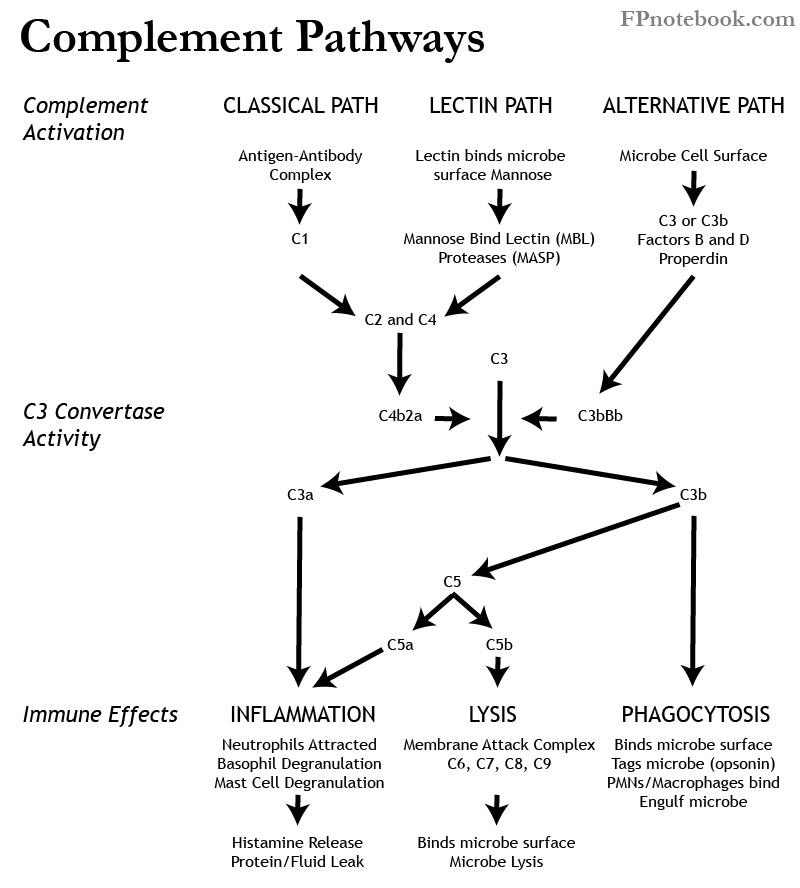
Complement Pathway
- Images
- Activation
- Classical Pathway (C1, C2, C3, C4)
- Alternate Pathway (Properdin, Factor B, Factor D, C3)
- Activation via Microbe cell surface
- Lectin Pathway (Mannose Binding Lectin or MBL)
- Mannose Binding Lectin (MBL) binds mannose on Microbe surface
- Mannose Binding Lectin Associated Proteases (MASP-1, MASP-2) are activated
- Classical Pathway (above) is stimulated
- Enzyme C3 Convertase (C3bBb or C4b2a) Formation
- Enzyme C3 Convertase splits C3 into C3a and C3b
- C3a stimulates inflammation (attracts Neutrophils, Histamine release)
- C3b stimulates Phagocytosis, inflammation (as with C3) and lysis (see below)
- Opsonization
-
Phagocytosis
- Phagocytes such as Neutrophils (PMNs) and Macrophages attract and engulf targeted organisms
- Inflammation (via C3a, C5a)
- Lysis
- Images


IV. Types: Adaptive Immunity
-
Humoral Immunity (B-Cells and Antibodies)
- Humoral Immunity (i.e. antibodies) targets extracellular pathogens
- B Cells
- Derivation
- Fetal Liver
- Bone Marrow Pluripotent Stem Cells
- Peripheral Migration to Secondary Lymphoid Tissue
- Spleen
- Lymph Nodes
- Peyer's Patches (Small Bowel)
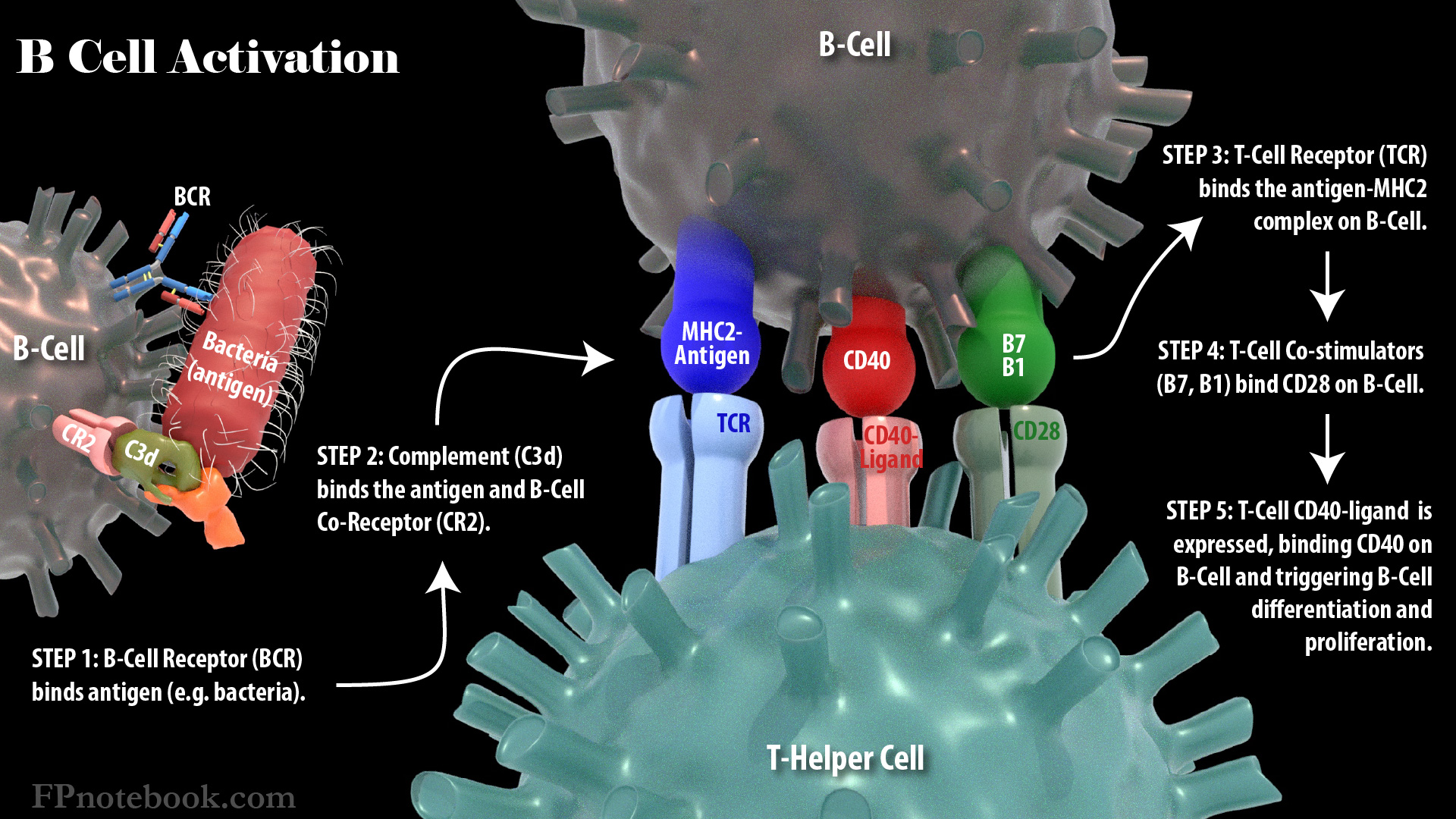
- Activation
- Images
- Recognition
- Antigen binds B-Lymphocyte Surface Receptor (BCR)
- BCR binding activates B-Lymphocyte
- B-Cell Proliferation
- Activated Lymphocytes proliferate
- B-Cell Differentiation
- Plasma Cells (Antibody producing cells)
- Survive for days to weeks producing antibodies, and without replicating
- Memory Cells
- Remain in B-Lymphocyte pool ready to respond to the same Antigen in future
- Future Antigen response is known as secondary immune response
- Plasma Cells (Antibody producing cells)
- Images
- Derivation
- Antibodies
- Images
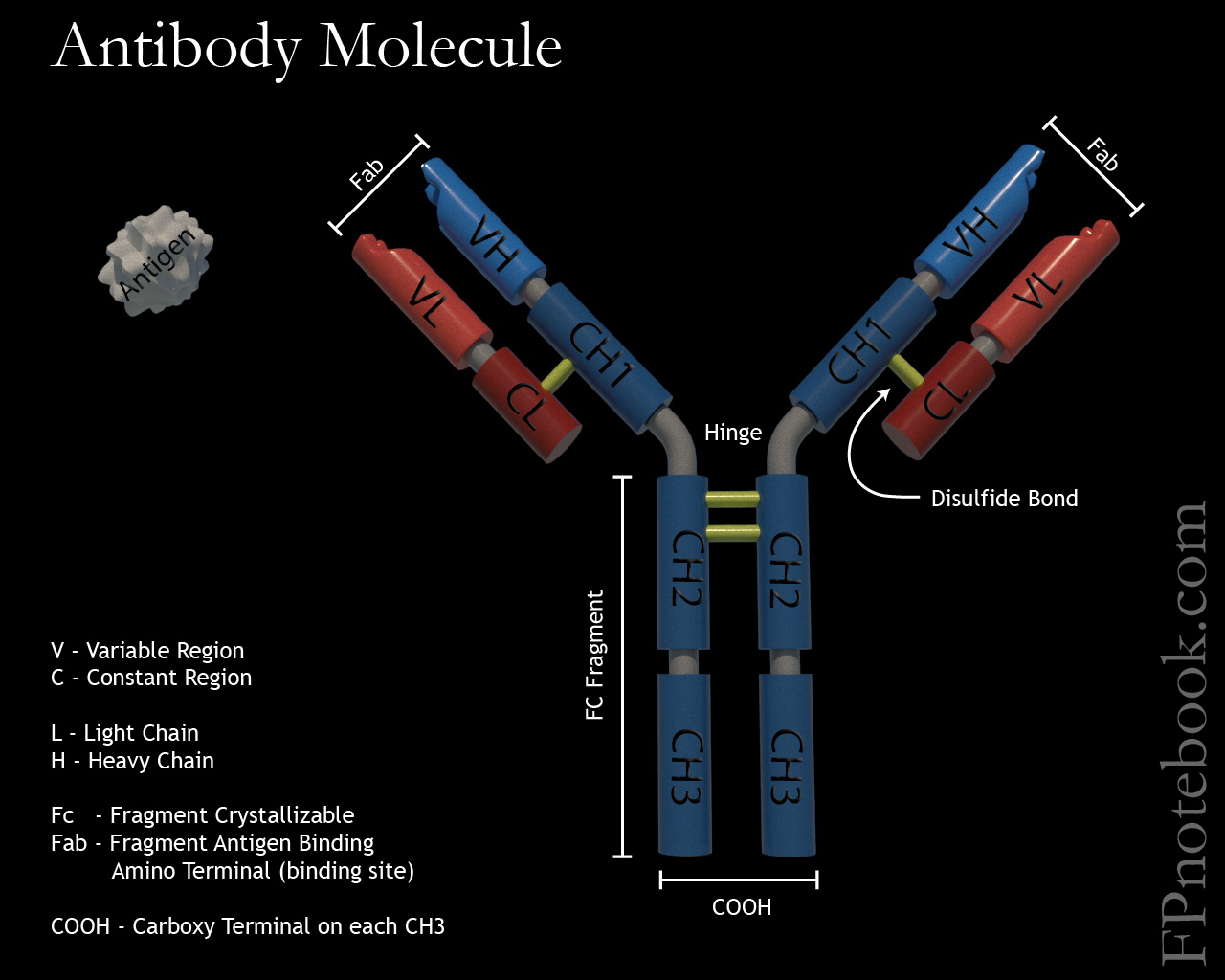
- Immunoglobulin (Ig)
- Immunoglobulins (or antibodies) are Y-Shaped Glycoproteins generated by Plasma Cells
- Immunoglobulin stem (Fc) is composed of 2 identical heavy chains
- Two Immunoglobulin Arms emanate from the stem
- Each arm is composed of 2 heavy chains and 2 light chains
- The end of each arm contains an Antigen binding site (Fab)
- Immunoglobulins have 2 forms
- Membrane bound Immunoglobulins (on surface of B-Cell)
- Secretory Immunoglobulin (unbound, free-floating)
- Monomeric antibodies exist as single Antibody molecules (IgE or IgG)
- Multimeric antibodies exist as multiple joined antibodies (IgA or IgM)
- Connected with J Chains
- Immunoglobulin G (IgG and subclasses IgG1-4)
- Monomer accounting for 75% of all Antibody, and has a serum Half-Life of 23 days
- Responsible for long lasting Immunity (secondary immune response) and Type 2 Hypersensitivity
- Immunoglobulin A (IgA and subclasses IgA1, IgA2)
- Immunoglobulin M (IgM)
- Immunoglobulin E (IgE)
- Long stem (Fc) monomeric Antibody with serum Half-Life of only 2.5 days
- Reacts to allergans (Type 1 Hypersensitivity) and Parasitic Infections
- Immunoglobulin D (IgD)
- Monomer with serum half life of 3 days
- Membrane bound surface Antibody
- Images
- Cell-Mediated Immunity (T-Cells)
- Cellular Immunity (i.e. T Cells) target Intracellular Pathogens (e.g. viruses and Intracellular Bacteria)
- T-Cells
- Derived in Bone Marrow
- Migrate to Thymus
- Maturation and Differentiation into two cell lines with different T-Cell Receptors (CD4 and CD8)
- Release into peripheral circulation
- T-Cell Surface Receptors
- T-Cell Receptors (TCR)
- Bind the Antigen on the Antigen Presenting Cell
- TCR Types
- TCR-alpha-beta (TCRab+)
- TCR gamma-delta (TCRgd+)
- T-Cell Co-Receptors
- CD4 binds MHC Class 2 - peptide/Antigen complex on surface of Antigen Presenting Cells (APC)
- Only Dendritic Cells, Macrophages, B-Cells (B-Lymphocyte) present MHC Class 2
- CD8 binds MHC Class 1 - peptide/Antigen complex on surface of Antigen Presenting Cells (APC)
- Any nucleated cell can present MHC Class 1
- CD4 binds MHC Class 2 - peptide/Antigen complex on surface of Antigen Presenting Cells (APC)
- T-Cell Receptors (TCR)
- T-Cell Types
- Effector Cells
- T-Helper Cells (CD4+ Cells)
- Releases Interferon
- Stimulates Phagocytosis by Macrophages
- Activates Natural Killer Cells
- Suppresses viral replication
- Releases interleuken 2
- Promotes T-Cell proliferation (esp. memory cells)
- Promotes B-Cell proliferation (memory cells and plasma cells)
- Releases Interferon
- T-Cytotoxic Cells (CD8+ Cells)
- Target and destroy tumor cells and virus-infected cells
- T-Helper Cells (CD4+ Cells)
- Other Cells
- Memory Cells
- Apoptosis of some cells not otherwise differentiated
- Effector Cells
- Naive T-Cell Activation

- T-Cell Receptor (TCR) binds to MHC-Antigen complex on Antigen Presenting Cells
- T-CellSurface CD28 binds to B7 Ligand on Antigen Presenting Cell
- T-CellSurface LFA-1 (Lymphocyte Function Associated Antigen) binds ICAM1 on Antigen Presenting Cells
- Interleukin-2 (IL2) produced by naive T Cells
- Stimulate T Cell proliferation

V. Pathophysiology: Inadequate Host Immune Response
- Infections
- See Bacterial Infection and Sepsis
- See Viral Infection
- See Parasitic Infection
- See Cutaneous Fungal Infection, Fungal Lung Infection, Candida Vulvovaginitis and Oral Candidiasis
- See Prion Disease
- Microorganisms adapt to host immune response
- Microorganisms may vary their Antigens or only trigger a weak Antigen immune response
- Bacterial encapsulation prevents Phagocytosis by Macrophages
- Bacterial cell wall may be resistant to immune-mediated lysis
- Bacteria may release toxins to counter or degrade host defenses
- Endotoxins (esp. Gram Negative Bacteria)
- Exotoxins (may damage Macrophages)
- Aggressins (increase Bacterial virulence, penetration, spread and persistence)
-
Immunodeficiency
- Primary Immunodeficiency
- Secondary Immunodeficiency (Acquired Immunodeficiency)
- Asplenism (e.g. splenectomy, Sickle Cell Anemia)
- Immunosuppressants
- Malnutrition
- Cancer involving Bone Marrow
- Radiation Therapy
- HIV Infection or AIDS (T Helper cell or CD4+ Cell infection)
VI. Pathophysiology: Exaggerated Host Immune Response
- Non-Hypersensitivity Reactions
- Schwartzman Reaction
- Excess Tumor Necrosis Factor induced by Bacterial Endotoxins resulting in shock state, DIC
- Excess Complement Activation (confirmed or proposed as mechanism in wide variety of conditions)
- Resistant infectious disease
- Hereditary Angioneurotic Edema
- Paroxysmal Nocturnal Hematuria
- Alzheimer's Disease
- Schizophrenia
- Atypical Hemolytic-Uremic Syndrome
- Macular Degeneration
- Crohn's Disease
- Tichaczek-Goska (2012) Adv Clin Exp Med 21(1):105-14 +PMID: 23214307 [PubMed]
- Cytokine Release Syndrome
- Sepsis-like systemic inflammatory reaction due to excessive systemic release of Cytokines by activated T-Cells
- Infections
- Acute Graft Versus Host Disease
- Chemotherapy
- Muromonab-CD3 (OKT3) Infusion
- Chimeric Antigen Receptor T Cell Therapy (CAR T-Cell Therapy)
- Other Conditions with Exaggerated Host Response
- Acute Respiratory Distress Syndrome (ARDS)
- Tumor Lysis Syndrome
- Hemophagocytic Lymphohistiocytosis (HLH)
- Macrophage activation syndrome (MAS)
- Schwartzman Reaction
-
Hypersensitivity Reaction (Gell and Coombs Classification, including autoimmune reactions)
- Type 1 - Immediate Hypersensitivity Reaction (IgE Antibody mediated)
- Immediate allergan immune response after repeated exposure (esp. in Atopic Patients)
- Examples
- Anaphylaxis (e.g. Penicillin)
- Urticaria
- Angioedema
- Anaphylactoid Reaction (e.g. Anaphylactoid Reaction to Radiocontrast)
- Atopic Allergy (e.g. Allergic Rhinitis, Allergic Asthma)
- Food Allergy
- Bee sting Allergy
- Allergic Occupational Asthma
- Type 2 - Cytotoxic Antibody Reaction (non-IgE Antibody Mediated Reaction)
- See Autoimmunity
- Mediated by IgG and IgM (on cell surface or extracellular complex) to specific Antigens
- Antibody-Antigen Complex destruction (Phagocytosis, Antibody cellular cytotoxicity or complement)
- Examples
- Transfusion Reaction (ABO Incompatibility)
- Rhesus Incompatibility (Rh Incompatibility, Autoimmune Hemolytic Anemia)
- Autoimmune Thrombocytic Purpura
- Hashimoto's Thyroiditis
- Grave's Disease
- Goodpasture's Syndrome
- Delayed transplant Graft Rejection
- Myasthenia Gravis
- Mycoplasma pneumoniae related cold Agglutinins
- Polyclonal Activation (triggered by Microorganism response, e.g. Trypanosoma cruzi)
- Type 3 - Immune Complex Reaction
- Antigen-Antibody immune complexes deposit in tissue (small complexes missed by Phagocytosis)
- Site of immune complex deposition determines effects (e.g. Vasculitis, nephritis, Arthritis)
- Examples
- Serum Sickness (prototypical Immune Complex Reaction)
- Systemic Lupus Erythematosus
- Erythema Nodosum
- Polyarteritis Nodosa
- Arthus Reaction (e.g. Farmer's Lung)
- Rheumatoid Arthritis
- Elephantiasis (Wuchereria Bancrofti reaction)
- Jarisch-Herxheimer Reaction
- Type 4 - Delayed-Type Hypersensitivity (Cell-Mediated)
- Reaction within 2-7 days after exposure
- Mediated by Effector T Lymphocytes (CD4+ and CD8+), activated in response to specific Antigens
- Examples
- Allergic Contact Dermatitis (e.g. Nickel allergy)
- Mantoux Test (PPD)
- Immune Allergic Contact Dermatitis after prior Mycobacterium tuberculosis exposure
- Type 1 - Immediate Hypersensitivity Reaction (IgE Antibody mediated)
VII. Prevention
VIII. Resources
- Immune System (Wikipedia)
IX. References
- Goldberg (2014) Physiology, MedMaster, Miami, FL
- Mahmoudi (2014) Immunology Made Ridiculously Simple, MedMaster, Miami, FL
- Guyton and Hall (2006) Medical Physiology, p. 419-50