
II. Epidemiology
- Ankle Fractures account for 15% of acute ankle injuries
III. Pathophysiology
- Ankle is an inherently unstable joint (esp. given Talus shape)
- Other risk factors
- High risk sports
- Increased Body Mass Index increases risk of ankle injury with less force
IV. Types
- Medial Ankle Fractures
- Isolated Medial Malleolus Fracture
- Distal Tibial Physis Fractures
- Distal Tibia Fractures are common Epiphyseal Fractures in Children
- Type 2 Salter-Harris Fracture
- Associated with external rotation, twisting injury in childhood sports
- Evaluate for associated transverse fibula Fracture
- Type 4 Salter Harris Fracture (Triplanar Fracture)
- Rare, axial loading injuries (e.g. fall) seen in teenagers
- High Risk Fractures for complication
- Three Fractures: Metaphysis, Physis (with alignment shift) and Epiphysis
- Anterior Ankle Fractures
- Anterior Tibial Physis Fracture (Type 3 Salter-Harris Fracture, Tillaux Fracture)
- Talar Neck Fracture (Pilot's Fracture)
- Historically seen in pilots involved in plane crash in which foot was forcefully pushed backward
- Primarily due to motor vehicle including motorcycle accidents
- Hawkins Classification 1-4 (dislocation seen in class 2-4)
- Osteonecrosis complicates Talar Neck Fractures in 21-58% of cases (esp. with higher Hawkins Class)
- Talar Dome Fracture
- Mechanism is typically inversion injury (e.g. Ankle Sprain) and may be misdiagnosed as Ankle Sprain
- Lateral Talar Dome Fractures
- Nearly always due to Trauma
- Tenderness at point anterior to the lateral malleolus (anterior-lateral talar dome)
- Medial talar dome
- May be atraumatic in some cases
- Tenderness at point posterior to the medial malleolus (posterior-medial talar dome)
- Lateral Ankle Fractures
- Distal Fibula Fracture or Lateral Malleolus Fracture (see Weber Classification below)
- Talus Fracture (Snowboarder's Fracture)
- Lateral Process Fracture of Talus caused by ankle dorsiflexion with foot inversion (unique injury to Snowboarding)
- Missed on 40-50% of Ankle XRays (confirmed on CT Ankle)
- Often initially misdiagnosed as Lateral Ankle Sprain
- Findings include significant swelling at lateral talus
- Delayed diagnosis risks malunion or nonunion, and subtalar degenerative Arthritis
- Whole Ankle Fractures
- Pilon Fracture (Tibial Plafond Fracture)
- Talus forced proximally and splitting apart the syndesmosis between the tibia and fibula
- Results from high energy Trauma with axial loading
- May also occur in the elderly, by low energy or rotational Trauma
- Intraarticular Fracture of the distal tibia at the ankle
- Associated with complicated Fracture patterns
- Requires CT Ankle (after Fracture reduction) to best define Fracture
- Risk for Compartment Syndrome
- Trimalleolar Fracture
- Accounts for 7-12% of Ankle Fractures
- Results from high impact injury (e.g. Collision Sports) or from fall
- Fracture of Medial Malleolus, Posterior Malleolus (posterior edge of tibia) and Lateral Malleolus
- Complex, unstable Fracture
- Surgical ORIF is often required unless well approximated closed reduction
- Pilon Fracture (Tibial Plafond Fracture)
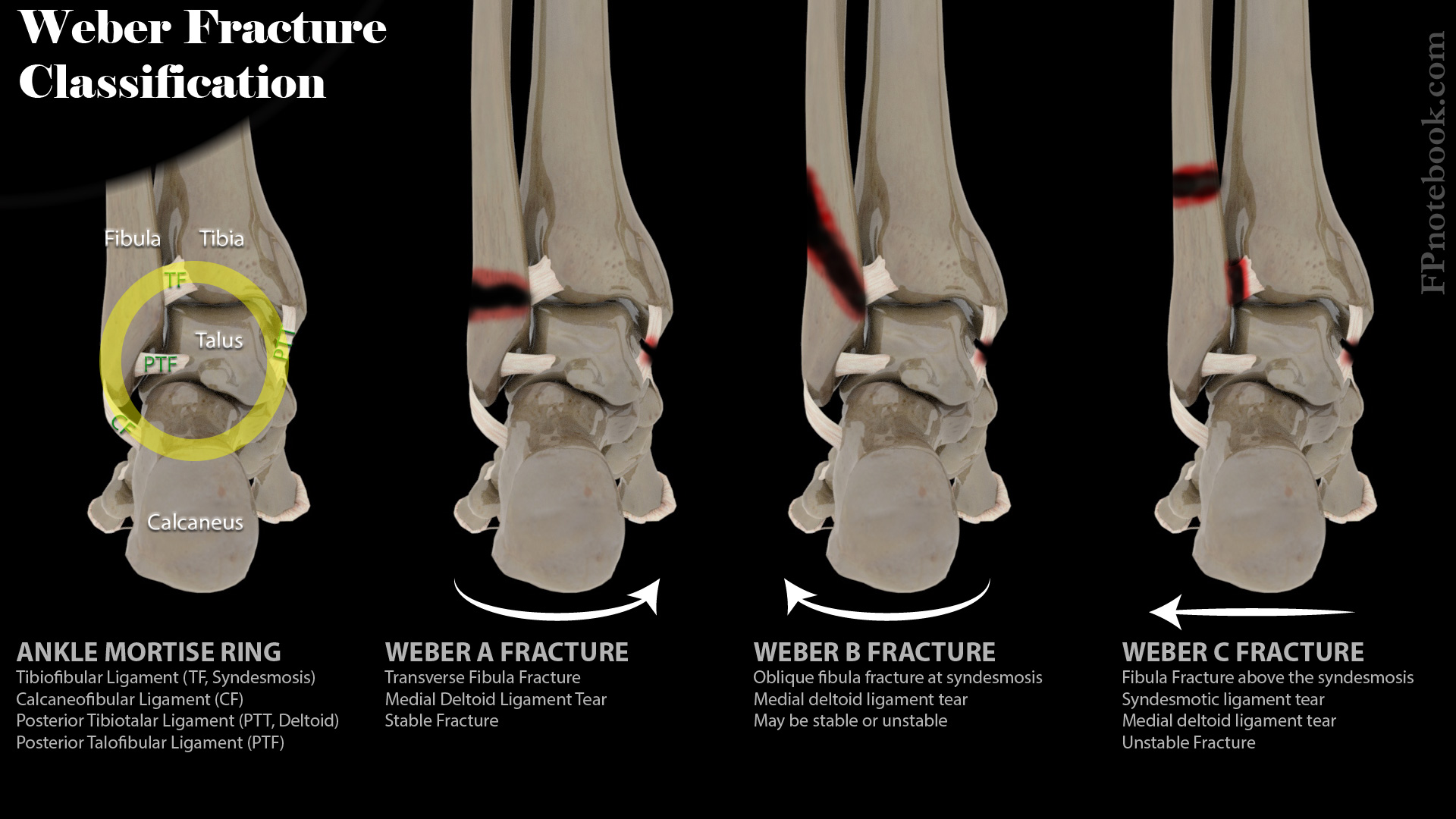
V. Classification: Fibula Fracture (Weber Classification)
- Precautions
- Weber Classification is a simplified classification system that does not rely on mechanism
- Weber Classification focuses on fibula Fracture site and relationship to the syndesmosis (DTFJ)
- Weber Classification under-evaluates the medial components
- Overall ankle stability is often more related to the medial component status
- Other Ankle Fracture classifications that focus on medial compartment are complex and rely on mechanism
- Closed Ring Classification (alternative classification)
- Ankle Joint is a closed ring held together by multiple ligaments (TF,PTF, CF, PTT, see image below)
- Two or more breaks in the ring are considered unstable
- Weber Classification is a simplified classification system that does not rely on mechanism
- Weber A (stable)
- Transverse fibula avulsion Fracture below syndesmosis and below talar dome and joint line
- May be associated with a medial malleolus Fracture (oblique or vertical) or medial deltoid ligament tear
- Infrasyndesmotic Fracture (below the distal tibiofibular joint or syndesmosis)
- Syndesmosis is intact
- Nearly always stable (esp. if no medial malleolus Fracture)
- Weber B (may be unstable)
- Fracture at the level of the talar dome
- Oblique fibula Fracture (spiral Fracture) at syndesmosis
- May be accompanied by medial deltoid ligament tear or medial malleolus transverse avulsion Fracture
- May tear anterior tibiofibular ligament (lateral ankle)
- Transyndesmotic Fracture (at the level of the distal tibiofibular joint or syndesmosis)
- Syndesmosis is typically intact
- Fracture is often unstable (esp. if medial Deltoid ligament rupture)
- Findings of instability
- Widening of the distal tibiofibular joint (DTFJ) or syndesmosis on (mortise view)
- Instability findings on ankle stress views (performed by orthopedics)
- Weber C (unstable)
- Lateral malleolus fibula Fracture, above ATF ligament
- Associated with Tibiofibular syndesmotic ligament rupture
- May be associated with transverse medial malleolus Fracture or medial Deltoid ligament rupture
- Suprasyndesmotic Fracture (above the level of the distal tibiofibular joint or syndesmosis)
- Weber C Fractures are always considered unstable until specialty evaluation
- Images
- References
VI. Exam
- See Ankle Exam
- See Knee Exam
- See Foot Exam
- Key exam points
- Key Tenet of all Musculoskeletal Exams: Neurovascular, Joint above, joint below, skin and compartments
- Thorough neurovascular exam of the foot
- Include exam and palpation of proximal tibia and fibula, and foot
VII. Findings: Signs and Symptoms
- Local tenderness and pain
- Tenderness over the medial deltoid ligament or medial malleolus may be associated with deltoid ligament injury
- Swelling
- Ecchymosis
- Inability to bear weight
- Significant deformity if dislocation present
VIII. Differential Diagnosis
IX. Associated Conditions
- See Calcaneal Fracture
-
Fifth Metatarsal Fracture
-
Jones Fracture
- Transverse Fracture at base of fifth Metatarsal at metaphysis due to inversion injury
- Pseudo-Jones Fracture
- Avulsion Fracture of base of fifth Metatarsal (at peroneus brevis insertion)
- Results from plantar flexion and inversion injury
-
Jones Fracture
- Maisonneuve Fracture (occurs in 1-11% of ankle injuries)
- Results from internal rotation of leg on fixed foot
- Findings include proximal fibula tenderness in addition to significant ankle injury
- Obtain Tibia-Fibula XRay if risk for Maisonneuve Fracture
- Findings suggestive of Maisonneuve Fracture
- Medial malleolar Fracture or deltoid ligament disruption without distal fibular Fracture
- Distal tibiofibular joint (syndesmosis) widening without a distal fibular Fracture
- Ankle Sprain with proximal fibula tenderness
- Multiple associated distal injuries at ankle
- Deltoid ligament rupture
- Anterior and posterior talofibular ligament rupture
- Syndesmotic ligament rupture
- Proximal injuries at knee
- Proximal tibiofibular ligament rupture or
- Proximal Fibula Fracture
- Risks
- Unstable Fracture if syndesmotic instability (consult orthopedics)
- Motor weakness due to superficial fibular nerve compression
- Associated with Compartment Syndrome
- Frequently missed on initial evaluation (always evaluate proximally in Ankle Fractures)
X. Imaging
-
Ankle XRay (AP, Lateral and Mortise View)
- See Ankle XRay
- Consider Foot XRay, Tibia-Fibula XRay or dedicated CalcaneusXRays
- Instability findings
- Widening of ankle mortise (Weber C and some Weber B Fractures)
- Consistent with unstable Ankle Fracture
- Consider performing on stress view in unimalleolar Fractures
- Lateral talus displacement at rest, on gravity stress or external rotation (Weber B)
- Suggests Deltoid ligament rupture (and unstable Fracture)
- Consistent with a "bimalleolar-equivalent" Fracture
- Unimalleolar Fracture with ligament instability at opposite malleolus
- Widening of ankle mortise (Weber C and some Weber B Fractures)
- Tib-Fib Xray
- CT Ankle
- MRI foot indications
- Suspected Calcaneal Stress Fracture or Navicular Stress Fracture
XI. Management: Initial emergency department evaluation
-
General measures
- Rest, elevation and non-weight bearing
- Ice to area up to every 20 min per hour while awake for first 72 hours
- Reduce Ankle Fracture-dislocation
- Do not delay reduction of dislocated ankle and displaced farcture
- Risk of tissue ischemia (including skin necrosis) and articular surface injury
- Perform reduction under Hematoma Block or Procedural Sedation
- Apply inline traction while Splinting (Quigley maneuver pulls great toe up and medially)
- Most Fractures requiring reduction will need surgical management
- Do not delay reduction of dislocated ankle and displaced farcture
- Initial Splinting
- Emergent orthopedic evaluation and surgery
- Open Fracture
- Neurovascular compromise
- Non-reducible Fracture
- Routine surgical management
- Indications
- Weber C Fracture
- Weber A Fracture with medial malleolus Fracture
- Trimalleolar Fracture
- Maisonneuve Fracture
- Weber B Fracture with instability (refer all Weber B Fractures to orthopedics for reevaluation)
- Findings suggestive of instability
- Ankle mortise wide
- Lateral talus displacement on gravity stress or external rotation
- Findings suggestive of stability (stable Fracture in 98% of cases if both criteria present)
- Posterior displacement of of distal Fracture fragment <2mm (on lateral XRay)
- Only two Fracture fragments
- Nortunen (2017) J Bone Joint Surg Am 99(6): 482-7 +PMID:28291180 [PubMed]
- Findings suggestive of instability
- Initial management
- Immobilize in fiberglass or plaster splint (sugar tong with or without posterior splint)
- Non-weight bearing and elevation
- Follow-up re-evaluation orthopedics for possible surgical management
- Weber B Fractures are indeterminate for surgical management until Stress Imaging
- ORIF may be performed in first day prior significant swelling, but otherwise after 6 days
- Indications
- Conservative Management
- Weber A Fracture without medial medial malleolus Fracture
- CAM Boot or hard-soled shoe
- Weight bearing as tolerated
- Fracture line may persist on xray despite asymptomatic patient (no management required)
- Distal fibular chip Fracture (ATF or CF Ligament avulsion Fracture)
- Treat with Ankle Sprain Management
- Weber A Fracture without medial medial malleolus Fracture
XII. Management: Lateral Ankle Fracture (Weber-based protocol)
- Surgical management (ORIF) Indications (disrupted ankle mortise)
- Non-surgical, conservate management
- Weber B Fracture with stable ankle mortise
- Weber A Fracture (stable Fracture)
XIII. Complications
- Ankle Osteoarthritis
- Osteoarthritis is more likely if poorly aligned ankle mortise or talus position
- Fracture management shoul ensure smooth articular surface of ankle
XIV. Prognosis
- Stable Fractures treated with non-operative, conservative therapy
- Return to baseline activity within 6-8 weeks is common
- Unstable Fractures requiring surgical intervention
- Weight bearing after surgery is often delayed up to 12-16 weeks
- Return to full functional capacity may require up to 2 years
- References
XV. References
- Courtney and Shannon (2020) Crit Dec Emerg Med 34(5): 14-5
- Kiel and Desvaristes (2019) Crit Dec Emerg Med 33(7): 16-7
- Orman and Ramadorai in Herbert (2017) EM:Rap 17(1): 7-9
- Titchner, Morris and Davenport (2021) Crit Dec Emerg Med 35(5): 17-23
- Tubbs and Janicki (2025) Adult Lower Extremity - Ankle, Mastering Emergency Imaging, CCME, accessed 5/10/2026