
II. Indications: Ottawa Ankle Rules in Acute Ankle Sprain (Over age 5 years old)
- Ankle XRay not needed if both are true:
- Able to ambulate at injury or in ER for 4 steps
- No pain over distal posterior 6 cm (2.4 inches) of tibia, fibula
-
Foot XRay not needed for mid-Foot Pain if both true:
- Able to ambulate at injury or in ER for 4 steps
- No pain at fifth Metatarsal base and Tarsal Navicular
- Efficacy
- Test Sensitivity for Malleolar Fracture: 95%
- Requires alert adult or child age 5 or older
- Injury within prior 10 days
III. Indications: Low Risk Ankle Rule (children over age 3 years old)
- Ankle XRay is not needed if:
- No marked swelling, deformity or malalignment AND
- No pathologic Fracture risk AND
- Tenderness is limited to distal fibula (distal to anterior tibial joint line) and lateral ligaments
- Efficacy
- Children must be over age 3 years old
- Finds high risk injury (e.g. distal tibia, proximal fibula, Ankle Dislocation) in 98-100% of those age >3 years old
- Misses nondisplaced distal fibula avulsion Fractures and Salter-Harris I and II Fractures
- References
IV. Technique: Views
- Anteroposterior Ankle
- Lateral Malleolus
- Medial Malleolus
- Talar Dome (talus)
- Tibial Plafond (distal tibia that articulates with the talar dome)
- Distal Tibiofibular joint (syndesmosis)
- Lateral Ankle
- Posterior Malleolus
- Talar Dome
- Oblique Ankle (Ankle Mortise View)
- Modified anteroposterior view perpendicular to the ankle mortise
- Leg internally rotated 15 to 20 degrees
V. Imaging: Pitfalls
-
Growth Plate Fracture in adolescent
- May be missed on Ankle XRay
- Consider if pain over lateral malleolus (fibula)
- Ankle Syndesmotic Sprain (High Ankle Sprain)
- Tibiofibular clear space widening >6 mm
-
Ankle mortise
- Space around the talus should be consistent (symmetric) at its margin between the tibia and fibula
-
Os Trigonum is a normal variant (lateral xray)
- Os Trigonum is an Ossification Center posterior to the talus
- Normal variant seen on lateral Ankle XRay in up to 14% of patients
-
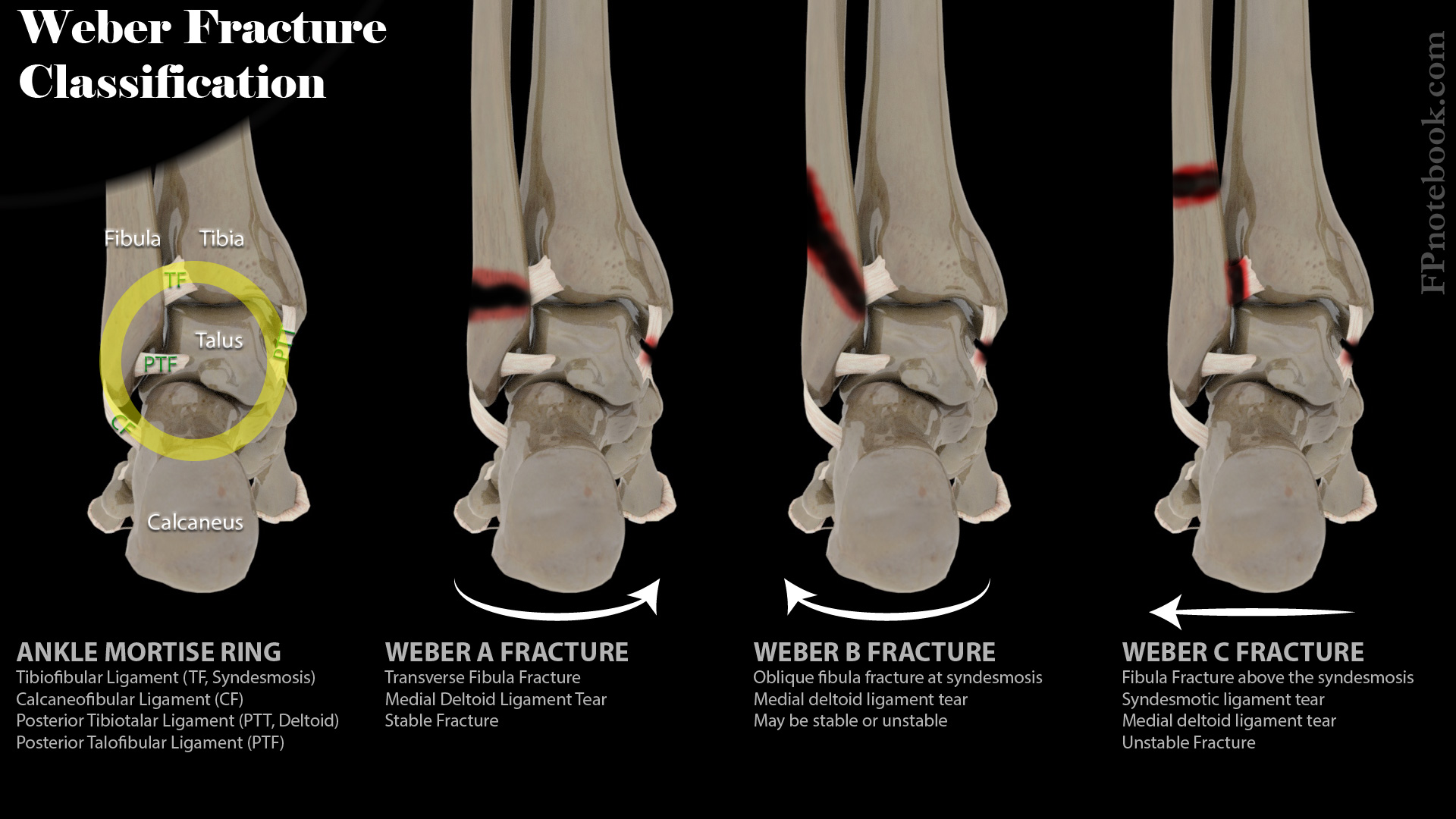
Ankle Fracture Stability (Weber A, B and C)

- See Ankle Fracture
VI. Evaluation
- See Musculoskeletal XRay ABCs (systematic XRay approach)
- Alignment and Adequacy
- Distal tibia and fibula should be visible
- Base of the fifth Metatarsal should be visible
- Bones
- Start distally, at bottom of film (work proximally up the film)
- Trace each bony cortex
- Review foot bones visible in film
- See Foot XRay
- Calcaneus and Talus
- Fifth Metatarsal base
- Review distal tibia and fibula
- Posterior malleolus
- Cartilage (Joint spaces)
- Ankle mortise with consistent spacing around the talar dome
- Distal tibial-fibular joint should overlap on mortise view
- Soft Tissue
- Ankle effusion (best seen on lateral ankle view)
- Fluid or hemarthrosis will appear more radiopaque (brighter white)
- Replaces the typical radiolucent (darker) fat the surrounds the joint (seen immediately adjacent to the joint line)
- Ankle effusion (best seen on lateral ankle view)
VII. References
- Tubbs and Janicki (2025) Adult Lower Extremity: Ankle, Mastering Emergency Imaging, CCME, accessed 5/10/2026
- Labovitz (1998) Foot Ankle Int 19:661-7 [PubMed]
- Stiel (1994) JAMA 271:827-32 [PubMed]