
II. Mechanism
- Central slip tears over PIP dorsum
- See Hand Anatomy
- Commonly occurs with ball striking dorsal finger
- Actively extended PIP joint forced into flexion
- Common basketball dislocation
- May also occur with volar dislocation of pip joint
- Images
III. Signs
- See Hand Injury
- See Hand Exam
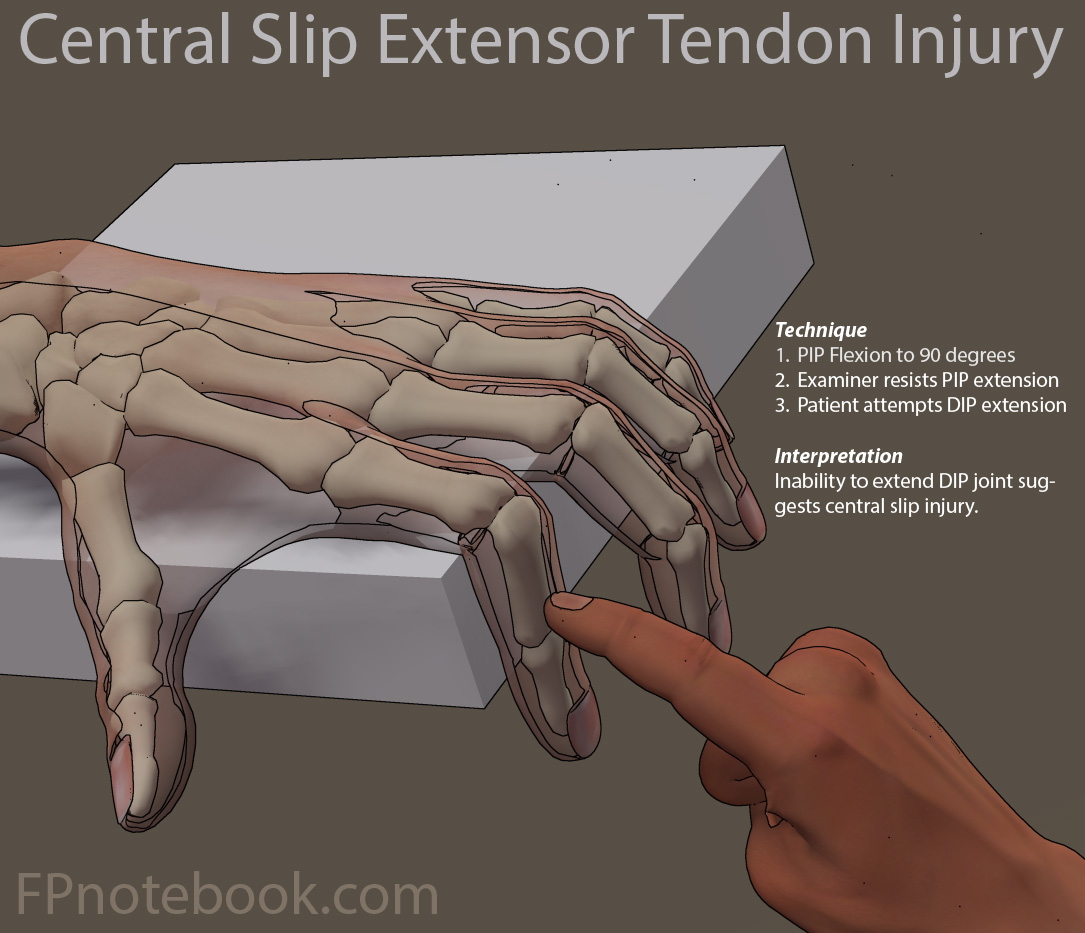
- See Elson Extensor Tendon Test
- PIP joint diffusely tender and swollen
- Maximal pain at midline dorsal proximal middle phalanx
- Pain on resisted finger extension
- Hold the PIP joint at 15-30 degrees flexion
- Patient unable to actively extend finger
- Passive extension still possible
- Inability to extend DIP joint when PIP is held in flexion

- Suggests central slip injury
- Assess for associated collateral ligament injury
IV. Imaging: XRay finger
- Normal in most cases
- Small proximal middle phalanx avulsion Fracture
V. Management
- Orthopedic referral indications
- Avulsion Fracture involving >1/3 of joint
- Passive extension of PIP not possible
- First 6 weeks
- Splint PIP joint in full extension
- Aluminum splint (do not use stack splint)
- Must maintain PIP extension continuously
- If PIP falls into flexion, 6 weeks starts again
- Daily passive range of motion of DIP joint
- May participate in sports if PIP remains splinted
- Splint PIP joint in full extension
- After 6 weeks
- Range of motion of PIP into full flexion
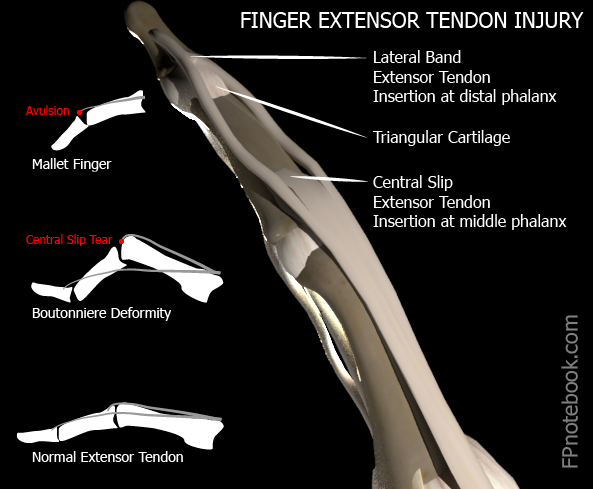
VI. Complications: Boutonniere Deformity
- Occurs when central slip injury not splinted
- Extensor slip lateral bands migrate to volar pip
- Develops weeks after initial injury
- Characteristics
- PIP Flexion contracture
- DIP and MCP hyperextension
VII. References
- Shamseldin (2003) AAFP Board Review, Seattle
- Leggit (2006) Am Fam Physician 73(5):810-23 [PubMed]