
II. Epidemiology
- Most common neonatal foot deformity
- More common in females
III. Etiology
- Results of positional confinement in utero
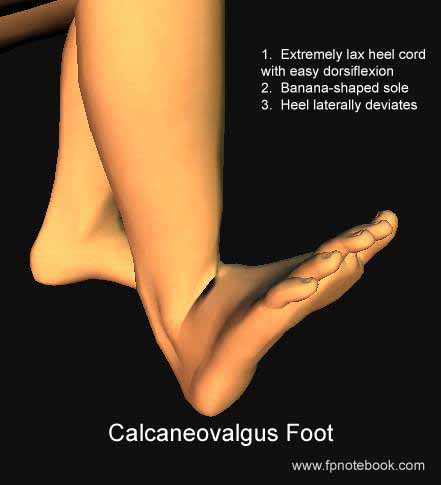
IV. Signs
- Images
- Easy to diagnose shortly after birth
- Foot has up and out appearance
-
Foot dorsiflexes easily (long heel cord, ligaments lax)
- Dorsiflex foot so toes touch anterior tibia
- Foot often held in extreme dorsiflexion
- Limited plantar flexion (less than 90 degrees)
- Lateral Sole deviation (banana shaped)
- Feet are everted (facing away from each other)
- Lateral Heel deviation
- View from behind with foot in dorsiflexion
- Heel position is valgus (medial malleoli are closer)
V. Differential Diagnosis: Severe, refractory calcaneovalgus
VI. Management
- Stretch child's foot
- Start as early as possible
- Gentle plantar flexion of foot with mild inversion
- Stretch dorsal tendons and ligaments
- Repeat frequently (e.g. at each diaper change)
- Firm, high-top lace up shoes or Splinting
- Indicated for cases refractory to Stretching
- Serial Corrective cast indications
- Foot remains severely deformed (rare)
VII. Prognosis
- Excellent overall prognosis
- Improves spontaneously and rapidly
- Partial correction results in a Flexible Flatfoot
VIII. Patient Resources
- Hughston Sports Medicine Foundation
IX. References
- Hoppenfeld (1976) Exam. Spine Extremities, p.159-60,223
- Churgay (1993) Am Fam Physician 47(4):883 [PubMed]
- Gore (2004) Am Fam Physician 69(4):865-72 [PubMed]
- Hoffinger (1996) Pediatr Clin North Am 43:1091-111 [PubMed]