
II. Epidemiology
- Upper extremity accounts for 5-10% of Deep Vein Thrombosis (DVT)
- Patients tend to be younger and of leaner body habitus than those with lower extremity DVT
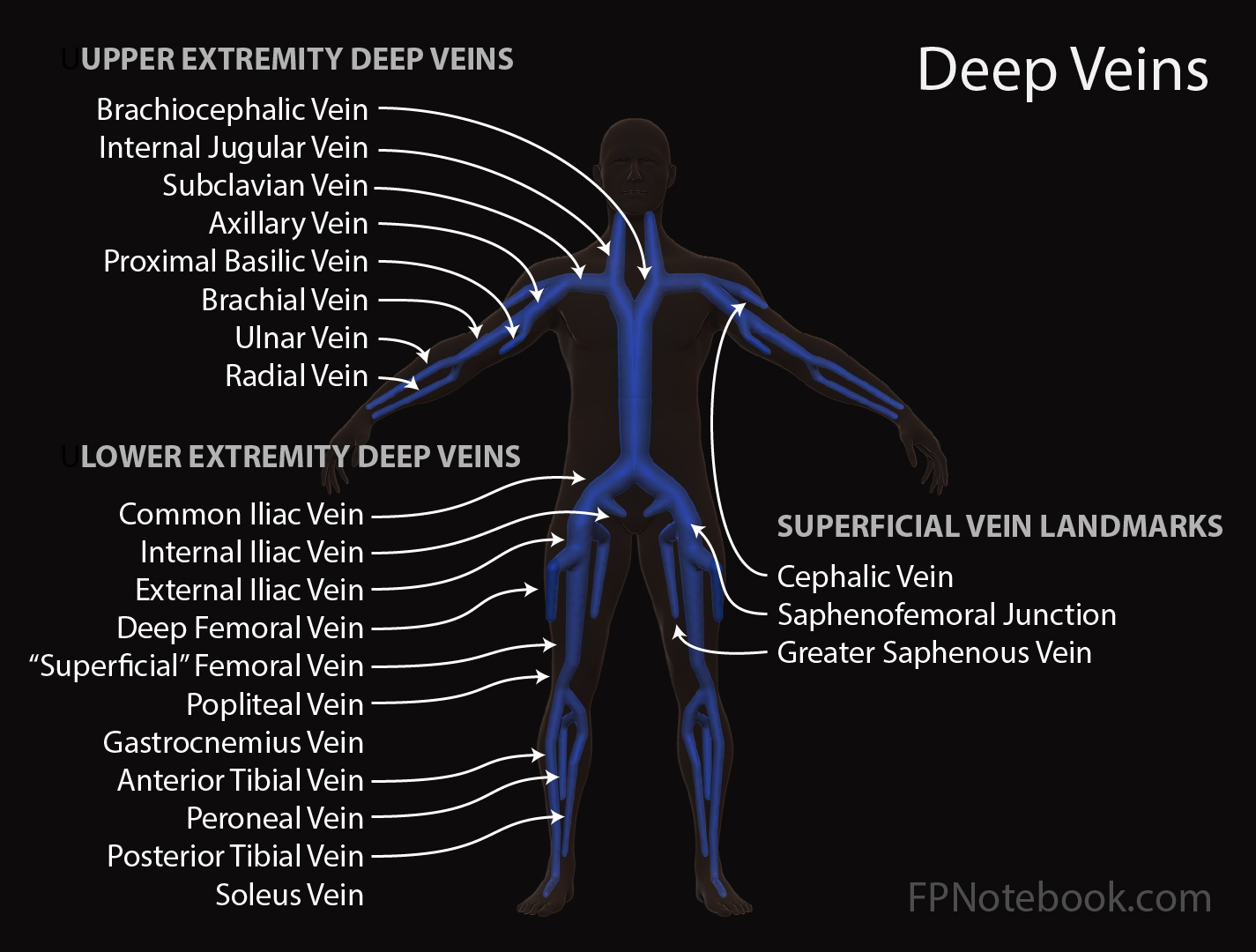
III. Anatomy
- Deep Veins of Arm
- Proximal Deep Veins
- Subclavian Vein (most common DVT site)
- Axillary Vein (common DVT site)
- Internal Jugular Vein (included in Upper Extremity DVT by some authors)
- Brachiocephalic Vein
- Distal Deep Veins
- Brachial Vein
- Radial Vein
- Ulnar Vein
- Proximal Deep Veins
- Superficial Veins of Arm
- Cephalic Vein
- Basilic Vein
IV. Causes
- Central Venous Catheter (common)
- PICC Line Thrombosis (complicates 3-5% of PICC Lines)
- Effort Thrombosis (Paget-Schroetter Syndrome)
- Incidence 1 to 2 per 100,000 per year in U.S.
- Venous form of Thoracic Outlet Syndrome
- Musculoskeletal swelling of axilla and upper arm results in external
- Compression interferes with arm venous outflow
- Occurs in athletes with upper extremity Muscle hypertrophy (rowers, swimmers, pitchers, tennis players, weight lifters)
- Overuse with hypertrophy of Scalene Muscles, especially in dominant arm
- Increased risk with congenital cervical ribs or subclavius ligaments
- Idiopathic (uncommon)
- Evaluate for occult cancer (up to 40% of Upper Extremity DVT causes)
- More likely than with lower extremity DVT
- Consider evaluation for Hypercoagulable state
- Evaluate for occult cancer (up to 40% of Upper Extremity DVT causes)
VI. Signs
- Arm with palpable cord
- Supraclavicular fullness
- Cyanosis or bluish discoloration of the extremity
- Serous drainage from PICC Line insertion site
- Venous distention
- Superficial vein distention (esp. chest wall and Shoulder)
- Jugular Venous Distention
VII. Differential Diagnosis
VIII. Imaging
- Images
- Duplex Ultrasound of upper extremity
- Test Sensitivity and Test Specificity approach 100% with skilled ultrasonagrapher
- Proximal subclavian vein may be difficult to image (clavicle shadowing)
- Advanced imaging options in indeterminate Ultrasound
- CT or MRI (timed for venous phase evaluation)
IX. Management: Proximal Upper Extremity Deep Vein Thrombosis
- Indications: Proximal Deep Vein Thrombosis
- Subclavian Vein Thrombosis
- Axillary Vein Thrombosis
- Internal Jugular Vein Thrombosis
- Brachiocephalic Vein Thrombosis
-
Anticoagulation
- See Anticoagulation in Thromboembolism
- Duration: Typically 3 months (6 months or longer may be required if persistent risk)
- Consider catheter directed Thrombolysis (severe acute edema, pain presentations)
- Large thrombus
- Acute within last 2 weeks
- Patients with low bleeding risk
X. Management: Distal Upper Extremity Deep Vein Thrombosis
- Indications: Distal Deep Vein Thrombosis
- Brachial Vein
- Radial Vein
- Ulnar Vein
- Approach
- Observation (typical) OR
- Prophylactic dose Anticoagulation OR
- Therapeutic dose Anticoagulation (high risk patients)
- Catheter-Associated Venous Thrombosis and catheter remaining in place (see below)
- Cancer patients with low risk of bleeding
XI. Management: PICC Line Venous Thrombosis
-
PICC Line venous thrombosis risk: 2.5%
- May present as serous drainage from the PICC insertion site
- New Recommendations
- PICC Line does not need to be removed in most Upper Extremity DVTs (if functional and ongoing need)
- Anticoagulate for 3 months regardless of presence of cancer (or as long as PICC in place if longer than 3 months)
- Older recommendations were to remove the PICC Line and not replacing (even if placed on opposite side)
- References
- (2012) Chest 141(2): e419S-e494S [PubMed]
- DeLoughery and Orman in Majoewsky (2012) EM:Rap 12(12): 4-5
- Jones (2010) J Vasc Surg 51(1):108-13 [PubMed]
XII. Complications
- Pulmonary Embolism (6% of cases; contrast with lower extremity DVT related PE of 33%)
- Post-thrombotic Symdrome (13% of cases)
- Superior Vena Cava Syndrome
XIII. References
- McCollom (2021) EM:Rap 21(8)
- Mintz and Levy (2017) Upper Extremity Deep Vein Thrombosis, ACC Website, accessed 8/6/2021
- Engelberger (2012) Circulation 126(6):768-73 +PMID: 22869858 [PubMed]
- Joffe (2002) Circulation 106:1874-80 [PubMed]
- Simon (2023) Am Fam Physician 107(5): 503-12 [PubMed]