
II. Protocol: Two Point DVT Ultrasound
- Interpretation
- Positive Focused Ultrasound
- Anticoagulate and arrange for formal comprehensive venous Ultrasound
- Negative Focused Ultrasound
- See Wells Clinical Prediction Rule for DVT
- DVT unlikely (Modified Wells Score <2)
- No further DVT testing needed
- DVT higher likelihood (Modified Wells Score >=2)
- D-Dimer negative
- No further DVT testing needed
- D-Dimer positive
- Arrange for formal comprehensive venous Ultrasound
- Anticoagulate if any significant delay in obtaining formal Ultrasound
- D-Dimer negative
- Positive Focused Ultrasound
- Precautions
- Wells Clinical Prediction Rule for DVT has wide discordance among providers (19% in this study)
- Two point Ultrasound does not assess for calf DVT
- References
III. Imaging: Two Point Focused Exam (by ER provider)
- Precautions
- This technique does not identify calf DVT
- Full venous Ultrasonography should be performed in all inconclusive cases with moderate to high suspicion
- Pearls
- In obese patients, compress untill artery starts to collapse
- Transducer
- Linear Array Transducer (5-12 MHz)
- Positioning
- Raise head of bed to 30-45 degrees
- Externally rotate leg
- Consider dropping leg over side of bed to help engorge veins
- Expose thigh and popliteal fossa
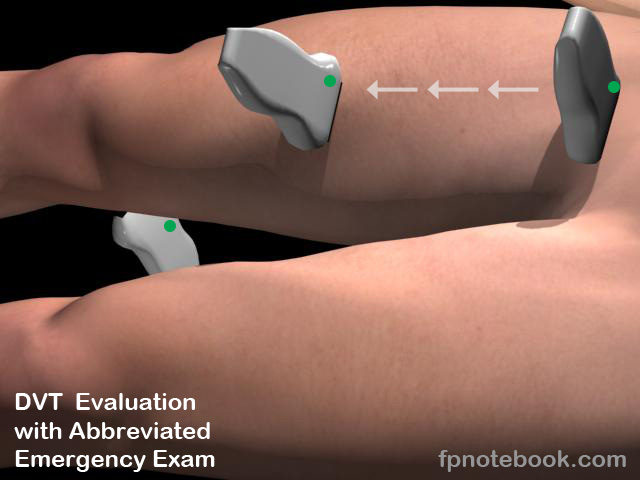
- Protocol evaluates vein compressibility and intravenous clot at a minimum of 3 waypoints
- Common Femoral Vein (near inguinal crease)
- Common Femoral Vein at confluence of greater saphenous vein
- Ideally perform compression at anterior thigh waypoints every 2 cm distally until unable to visualize
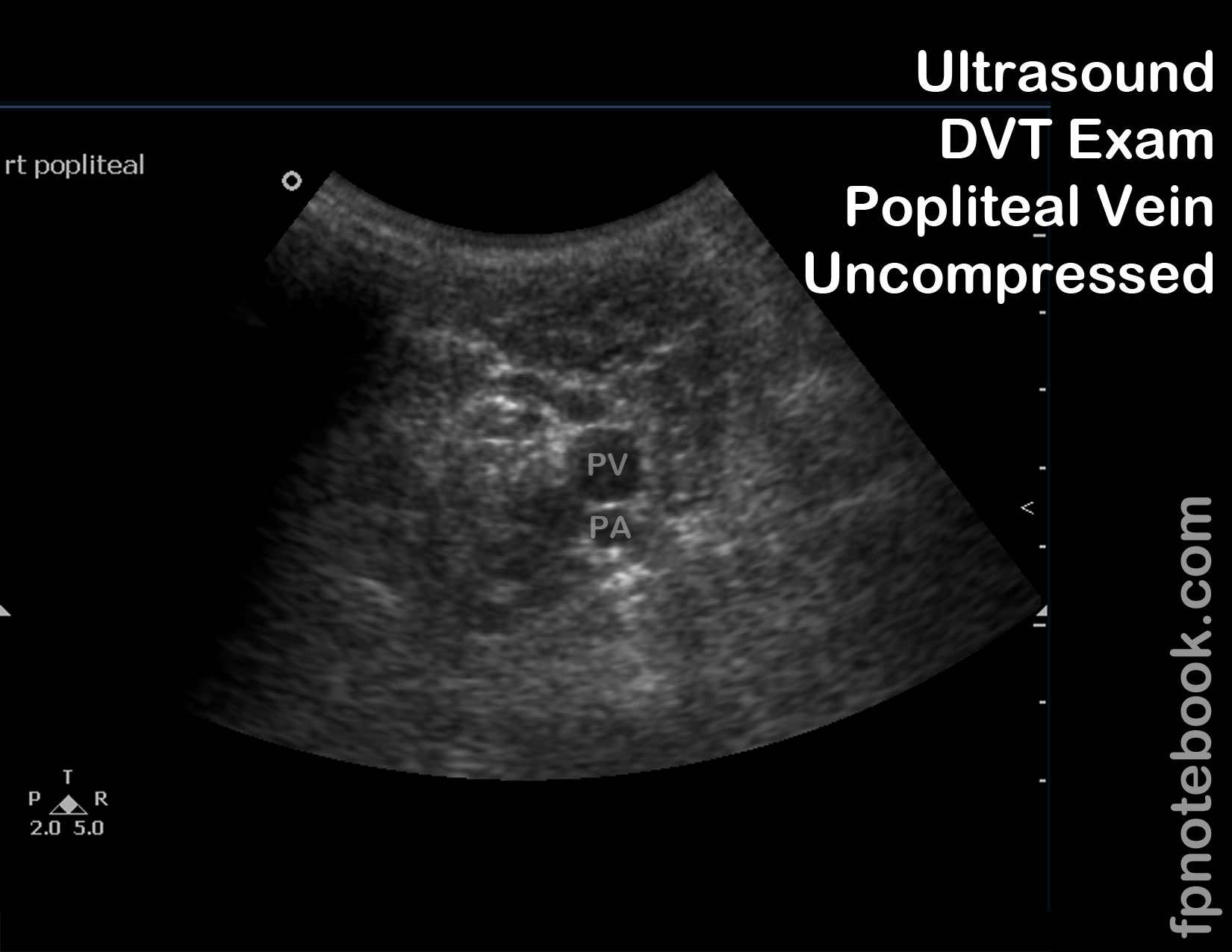
- Popliteal Vein (posterior to knee)
- Images
- Start position: Proximal Thigh
- Immediately below inguinal ligament
- Transducer is transverse (in short axis)
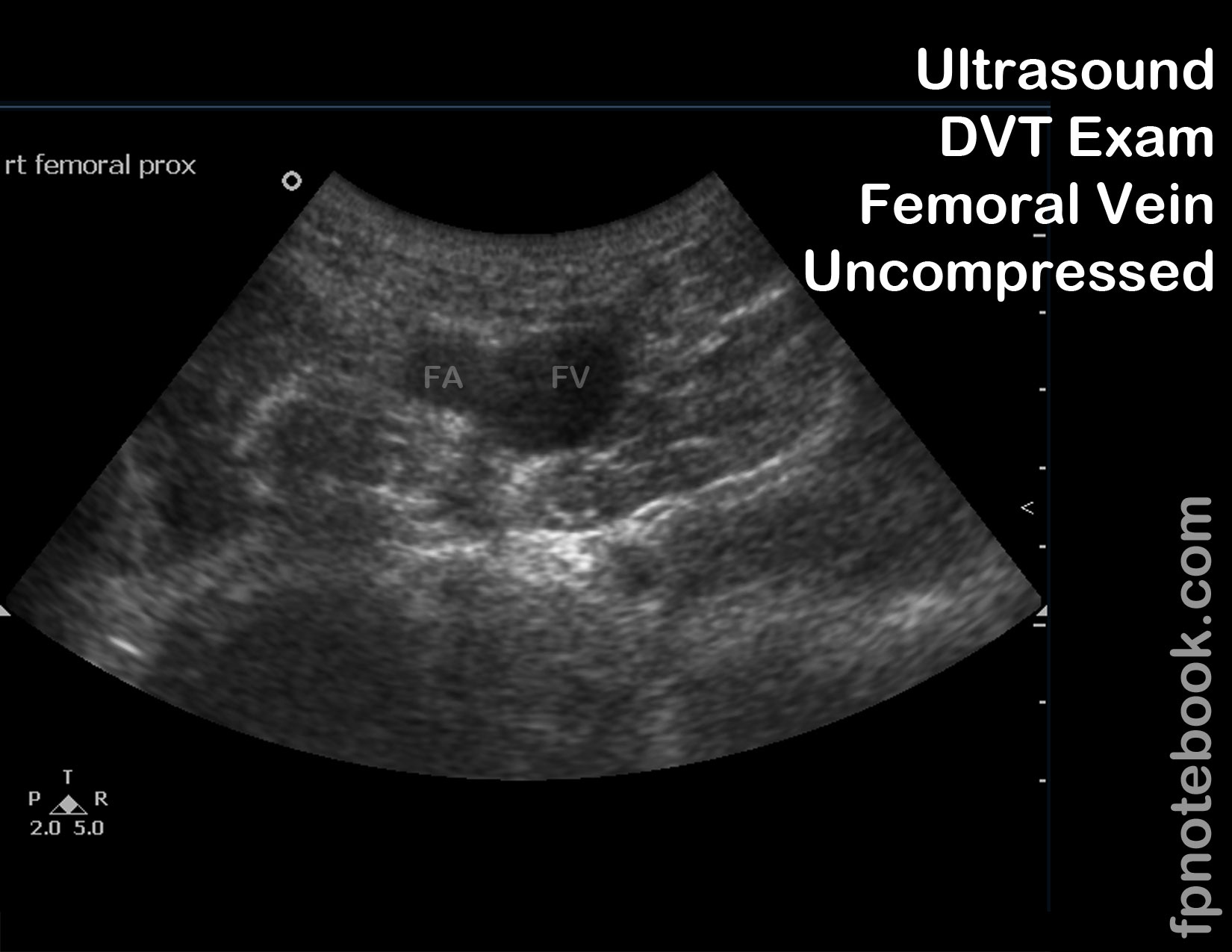
- Common Femoral Vein starts medial to femoral artery
- Moving distally, common femoral vein lies deep (posterior) to femoral artery
- Technique: Anterior upper leg
- Move distally down the course of the femoral vein in 1 cm increments (for 5-10 cm length)
- Greater saphenous vein will intersect the common femoral vein within a few centimeters of the inguinal ligament
- Femoral vein will become more difficult to visualize as the medial knee is approached
- Examiner may place opposite hand beneath the distal-medial thigh to improve visability
- Continue anterior examination until just below the bifurcation into superficial and deep femoral veins
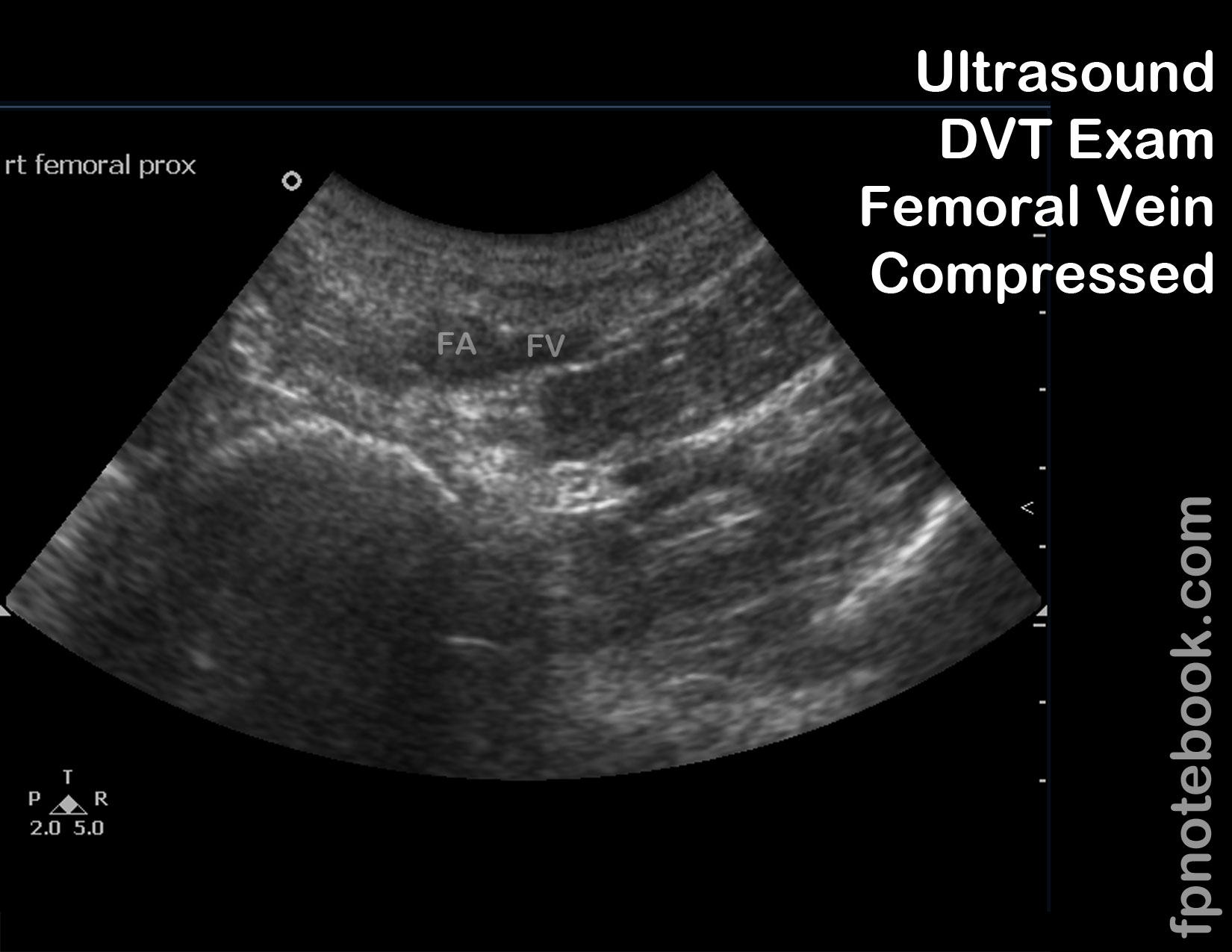
- At each femoral vein cross section (with femoral artery in the same view)
- Demonstrate that the femoral vein can be fully compressed
- Only accurate if compression is 90 degrees to the vessel (vessel may not compress with oblique pressure)
- Non-compressible vein suggests DVT
- Echogenic material may be seen within the vessel in a DVT present at least 5 days
- Consider using dual screen, one side with uncompressed vein and the other with compression
- Document with a continuous video or frozen images
- Demonstrate that the femoral vein can be fully compressed
- Move distally down the course of the femoral vein in 1 cm increments (for 5-10 cm length)
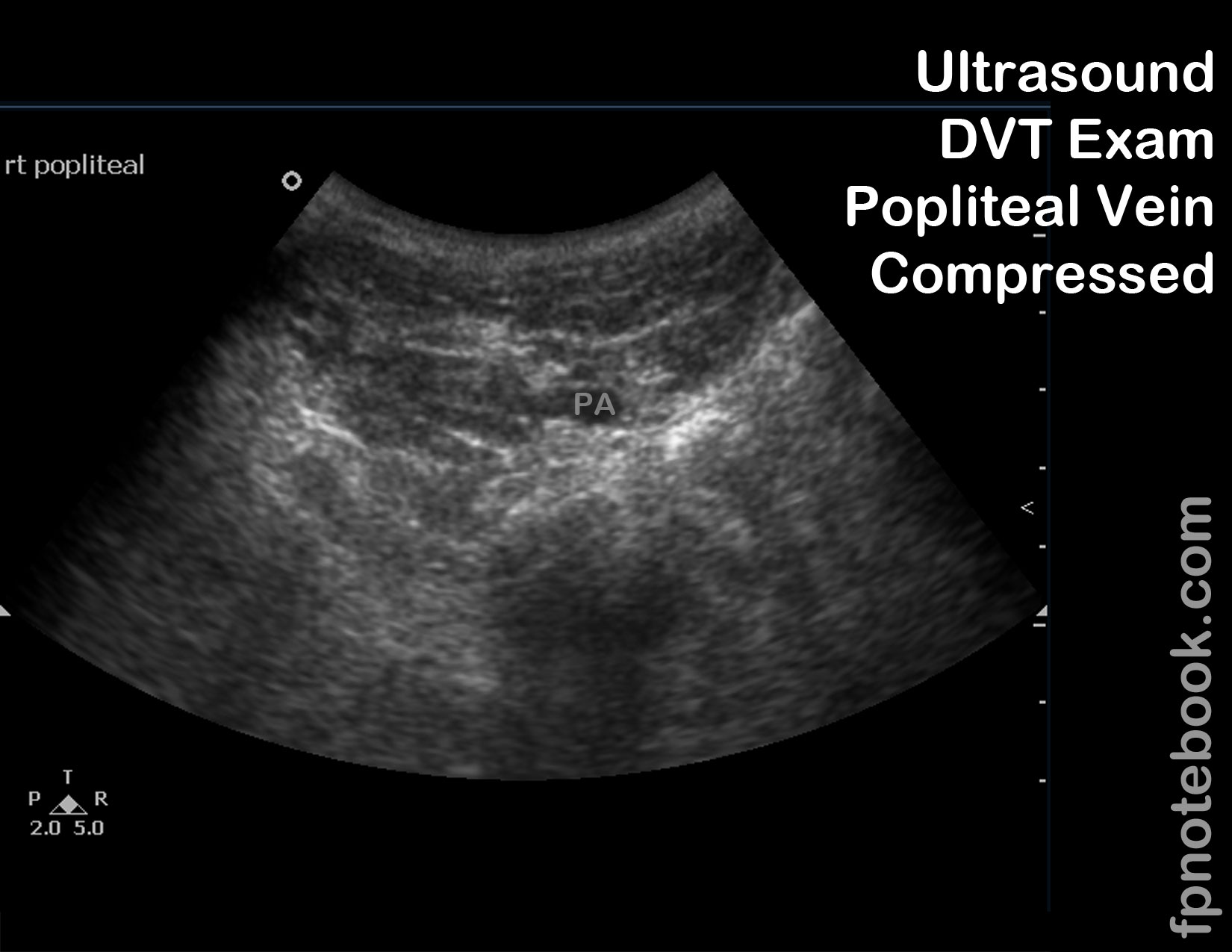
- Technique: Posterior leg from popliteal space inferiorly
- Identify the popliteal artery and vein in the popliteal space
- Continue to compress and release pressure on the popliteal vein for several centimeters below the popliteal space
- Technique: Augmentation (distal and proximal) - Optional
- Venous flow normally varies with respiration
- Augmentation of venous flow normally occurs when the calf is compressed and released or the Abdomen is compressed
- Visualize flow variation with color doppler (best seen when the vein is viewed longitudinally)
- Vein with DVT will lose its respiratory variation in flow and the augmentation effect with distal and proximal augmentation
- Iliac DVT (e.g. pregnancy) may be identified if femoral vein fails to vary in flow with respiration (may indicate Pelvis CTA)
- Calf thrombus may be identified on distal calf compression due to lack of augmentation (may indicate follow-up exam or calf Ultrasound)
- Documentation: Document fully compressible vein at two levels minimum
- Proximal femoral vein (with greater saphenous branch visualized)
- Popliteal vein

IV. Efficacy: DVT diagnosis by standard Compression Ultrasonography (by experienced Ultrasound tech)
- Symptomatic patient with unilateral proximal lower extremity swelling
- Test Sensitivity: 89-96%
- Test Specificity: 94-99%
-
False Negatives
- Test Sensitivity falls to <50% for asymptomatic proximal DVT
- False Negatives also seen with calf DVT, Upper Extremity DVT or pelvic vein thrombosis
V. Efficacy: Emergency and Primary Care Providers
- Accuracy improves to nearly 100% when Ultrasounds are repeated (typically at 1 week, esp. calf DVT)
- Focused two point, Point of Care Ultrasound (femoral, popliteal)
- Emergency Providers
- Primary Care Providers
VI. Resources
- Limited Assessment of Lower Extremity Venous System for Deep Vein Thrombosis (DVT) Video
- How to: Lower Extremity Deep Vein Thrombosis with Ultrasound (Sonosite)
VII. Advantages
- Can be done in the office setting
- Ultrasound is highly sensitive for deep vein thrombi
VIII. Disadvantages
- Ultrasound is not sensitive for detecting thrombi in calves
IX. References
- Derr (2012) Introduction and Advanced Emergency Medicine Ultrasound Conference, GulfCoast Ultrasound, St. Pete's Beach
- Reardon (2013) Emergency Ultrasound Course, 3rd Rock Ultrasound, Minneapolis, MN
- Noble (2011) Emergency and Critical CareUltrasound, Cambridge University Press, New York, p. 173-89
- Reardon (2011) Pocket Atlas Emergency Ultrasound, McGraw Hill, New York, p. 239-58