
II. Images
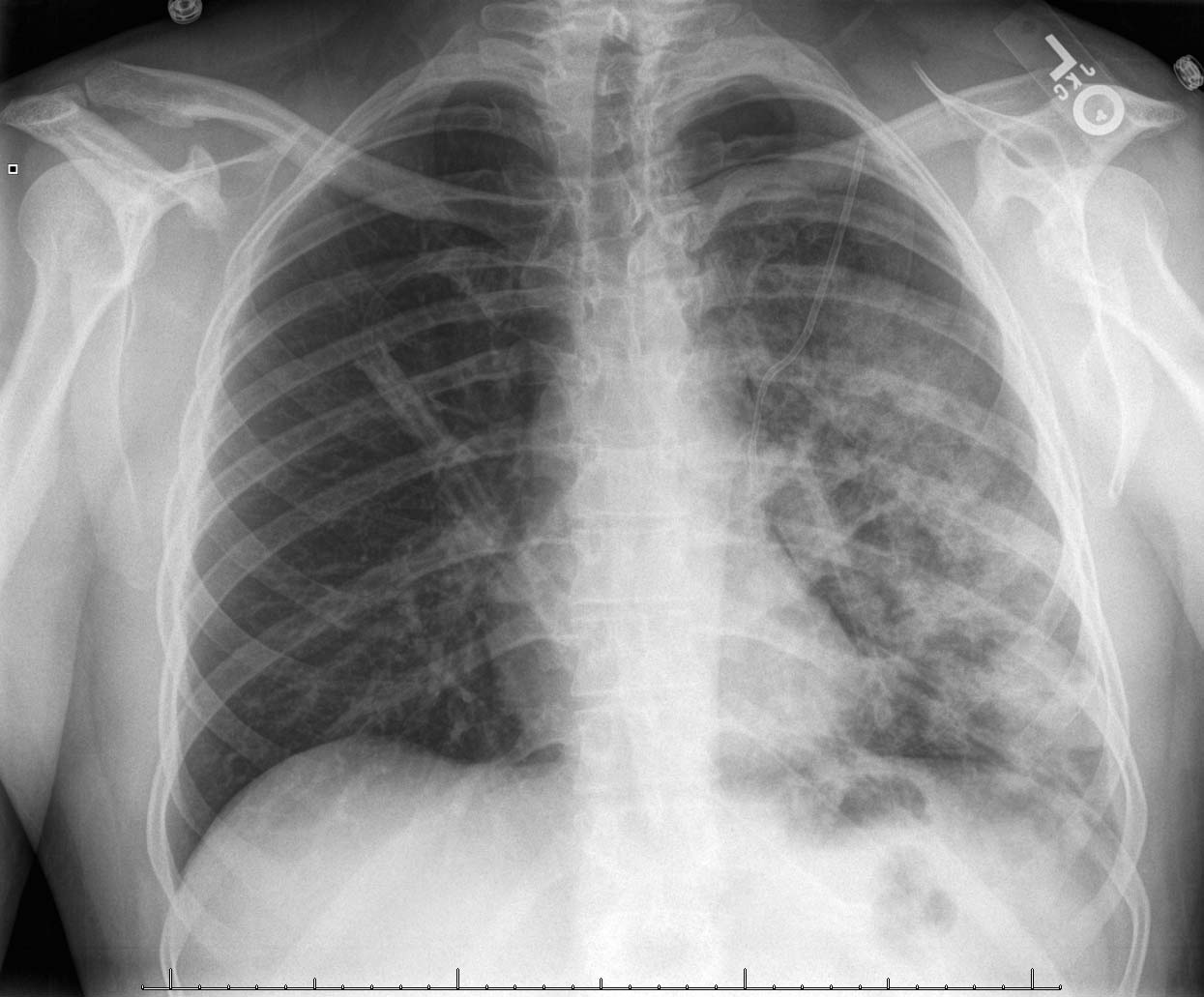
- Complete Pneumothorax
- Reexpansion Pulmonary Edema following Chest Tube placement

III. Imaging: Chest XRay
- Findings
- Medial
- Thin, line representing visceral pleura
- Interspace
- Radiolucent band without lung markings, typically at the apex on upright film
- Air-fluid level may be present (assume Hemothorax in Trauma)
- Lateral
- Chest wall
- Medial
- Posteroanterior (PA) Standard View - Inspiratory
- Best overall XRay to view to identify Pneumothorax
- Obtain upright image, as supine Chest XRay is unreliable and likely to yield a False Negative study
- Inverting the image (digitally reversing white-black) may highlight Pneumothorax lines
- End Expiratory views were used in past to enhance Pneumothorax
- Theoretically should enhance the Pneumothorax which is constant, by reducing the air in lung
- In practice, may add little additional diagnostic value to that seen on inspiratory films
- Lateral decubitus view (affected side up)
- May identify a small Pneumothorax suspected but not seen on upright Chest XRay
- Supine AP Portable XRay (Trauma)
- Unilateral deep sulcus sign at the costophrenic angle (laterally)
- Lung will appear hazy and indistinct (air rises anteriorly on a supine view)
- Apical pleural line will not typically be seen on supine view
- Heart border may appear very sharp on the side of Pneumothorax on a supine view film
- Criteria for large Pneumothorax
- British Thoracic Society
- Band or rim around lung margin of 2 cm or greater (50% pleural volume)
- American College Chest Physicians
- Apex to Cupola distance >3 cm (15-20% of pleural volume)
- British Thoracic Society
- Efficacy
- Test Sensitivity: <85% (compared with CT Chest)
- Lateral Decubitus XRay: 88%
- Upright PA CXR: 59%
- Supine AP CXR: 37%
- Test Sensitivity: <85% (compared with CT Chest)
-
False Positives
- Pulmonary Bleb (COPD) - may require CT Chest to distinguish
- Skin folds
- Scapula border
IV. Imaging: Advanced
-
Ultrasound chest
- See Lung Ultrasound for Pneumothorax (Sliding Lung Sign)
- Test Sensitivity 94% and Test Specificity 100% for Pneumothorax
-
CT Chest
- Gold standard in Pneumothorax
- Even large pneumothoraces on CT may be missed on Chest XRay
- Rodriguez (2019) Ann Emerg Med 73(1):58-65 +PMID:30287121 [PubMed]
- Indicated where Chest XRay cannot distinguish bleb in COPD from Pneumothorax
- In those with Secondary Spontaneous Pneumothorax due to blebs, contralateral blebs are seen in >50% of cases
- These contralateral blebs have a 25% chance of future secondary Pneumothorax
- May identify a clinically insignificant Pneumothorax that would resolve without treatment
- Identifies other associated thoracic Traumatic Injury
- Gold standard in Pneumothorax
V. References
- Noppen (2003) Respiration 70(4): 431-8 [PubMed]
- Majoewsky (2012) EM:RAPC3 2(2): 3-4
- Tranchell (2013) Crit Dec Emerg Med 27(7): 11-8