
II. Definitions
- Forearm Fracture
- Mid-shaft Fracture of the radius and/or ulna
III. Epidemiology
- Forearm Fractures (radius and/or ulna) are the most common Fractures of the upper extremity
- Distal Forearm Fractures (esp. Distal Radius Fracture) are most common
- Distal Radius Fractures peak age distribution is bimodal age (age <18 years and age >65 years)
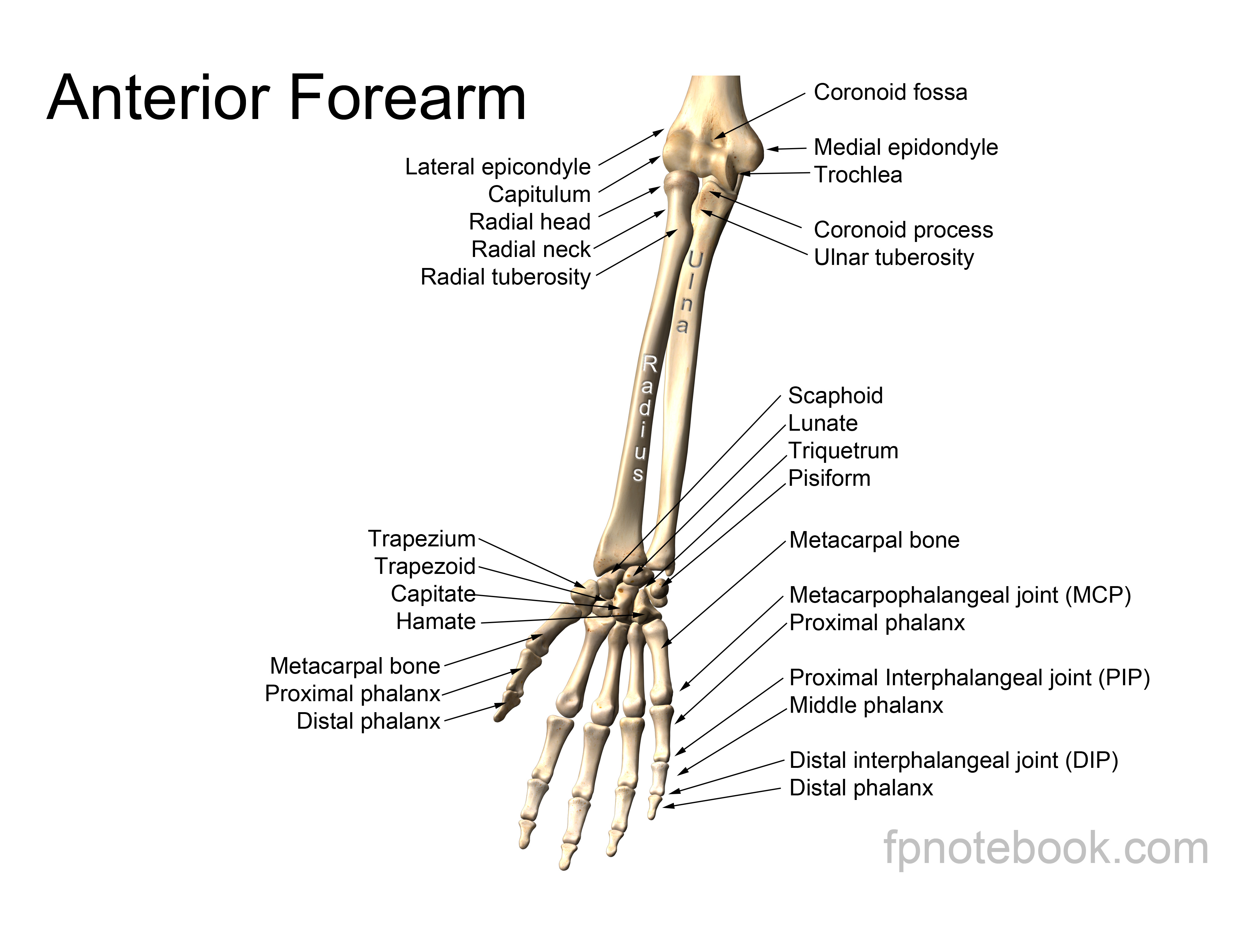
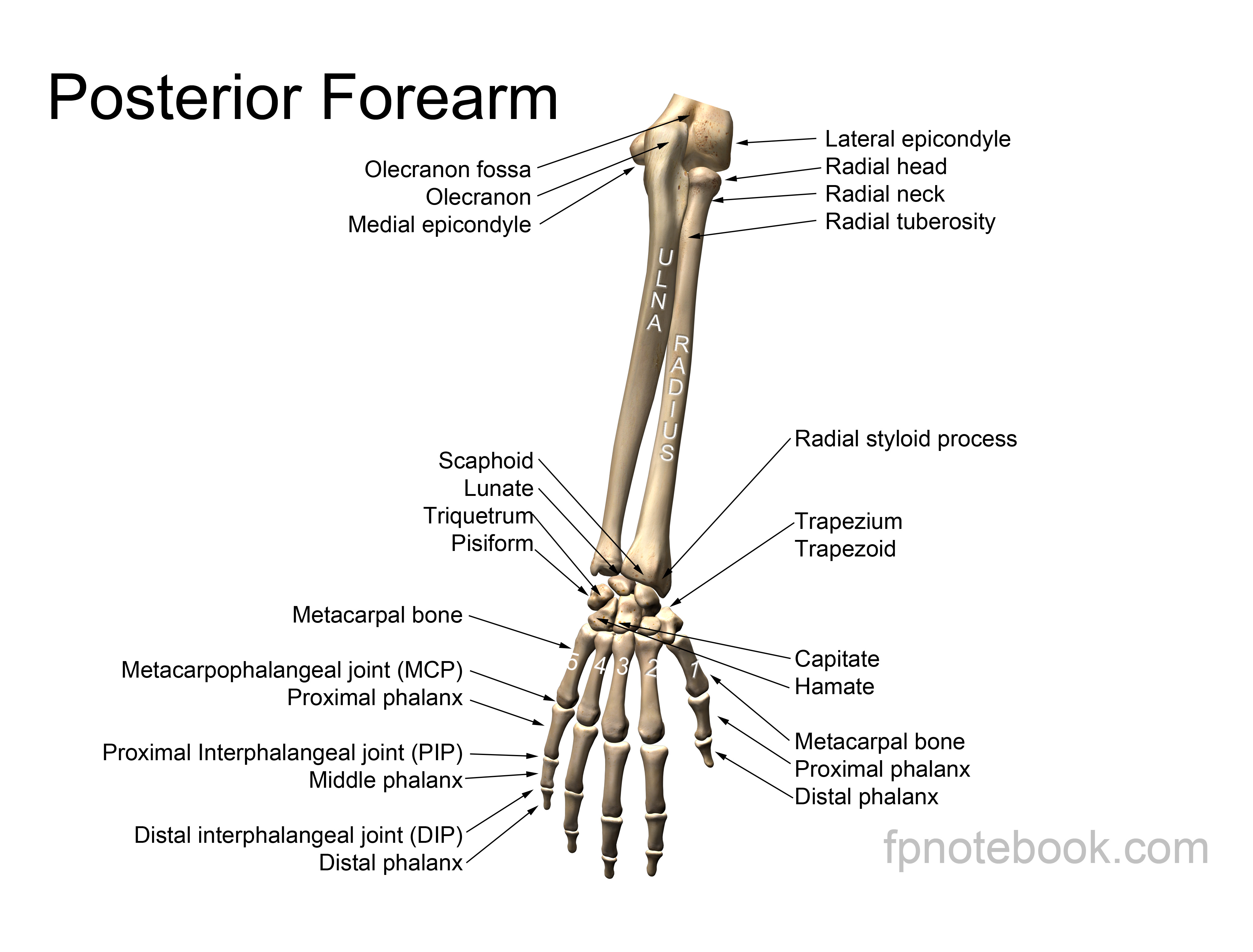
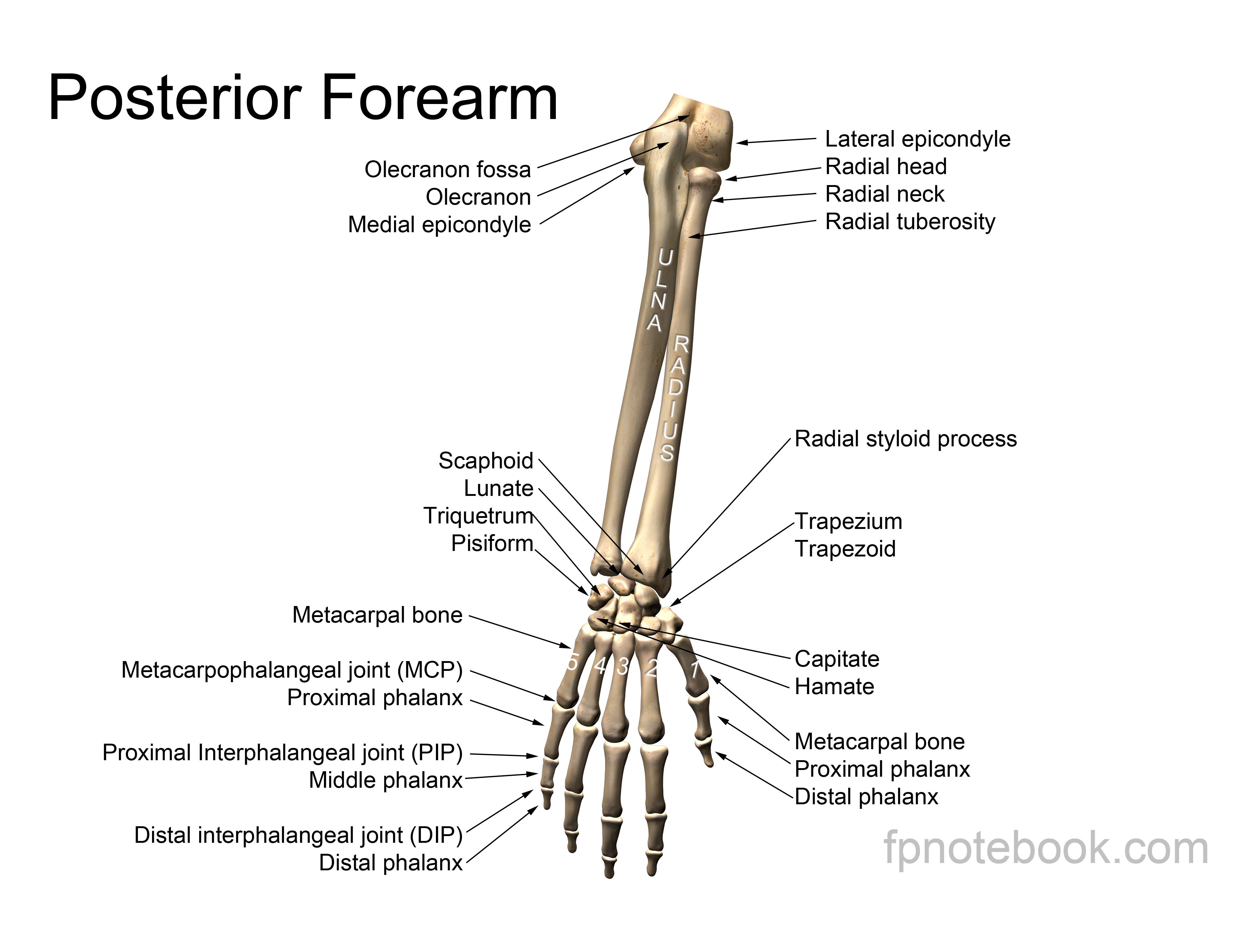
IV. Anatomy
- See Forearm Anatomy
-
Forearm rotation primarily involves radius rotating around the ulna (which is fixed due to olecranon)
- Radius and ulna are connected midshaft by an interosseous membrane
- Radius and ulna also form both proximal and distal joints
- Proximal Radio-ulnar joint (PRUJ): Radial Head and ulna's coronoid process
- Distal Radioulnar Joint (DRUJ): Distal Radius and Distal Ulna
-
Forearm is a ring structure of 2 bones attached at each end (elbow and DRUJ at wrist)
- One Fracture of the ring, makes a second Fracture or dislocation more likely
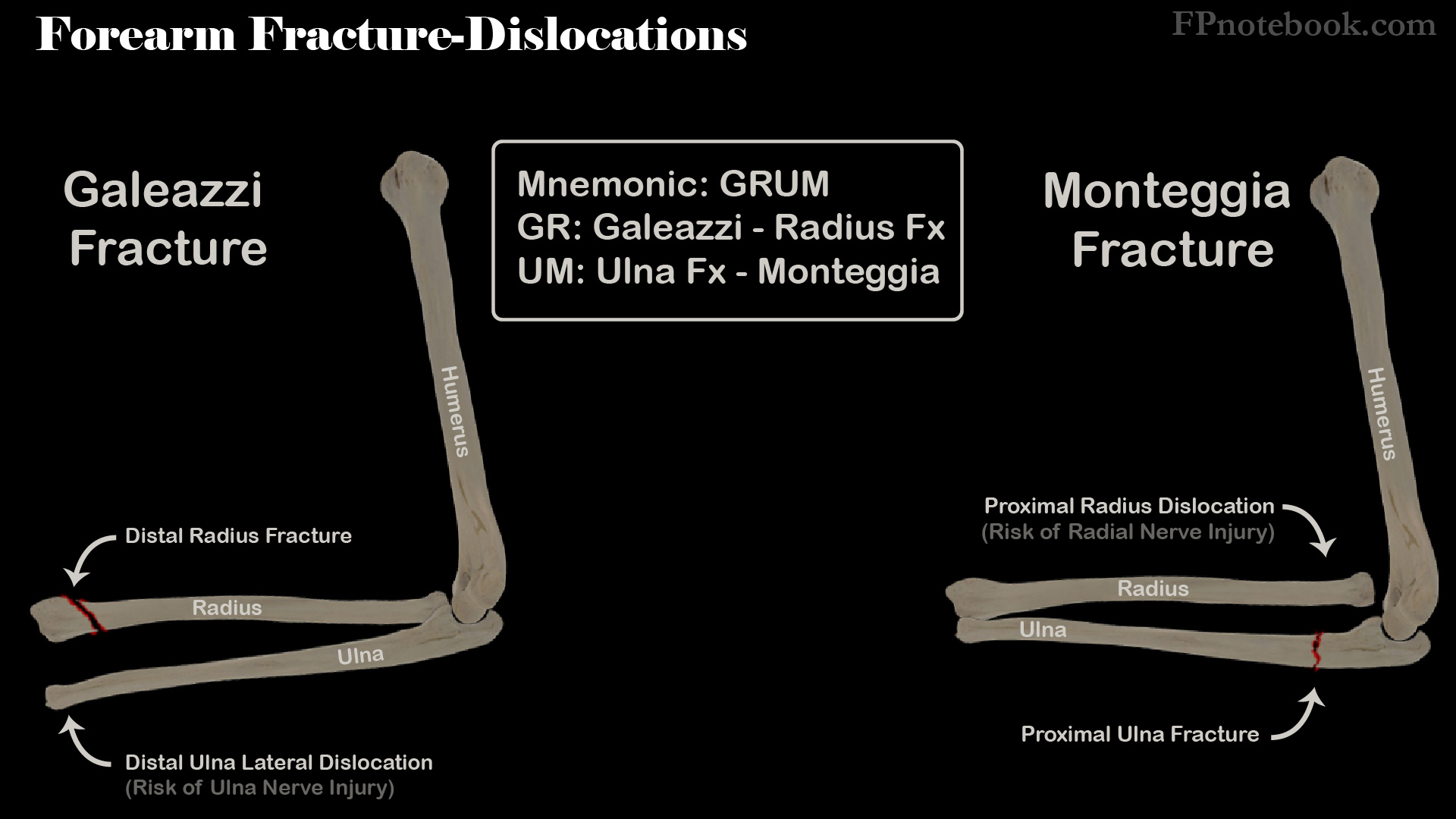
- Fracture dislocations include Galeazzi Fracture, Monteggia Fracture
- Images
 Also available as a Poster size image. See printing instructions and image restrictions.
Also available as a Poster size image. See printing instructions and image restrictions. Also available as a Poster size image. See printing instructions and image restrictions.
Also available as a Poster size image. See printing instructions and image restrictions.
V. Mechanism
- Fall on an outstretched hand (axial loading) is the most common mechanism of Forearm Fracture
- Isolated midshaft Ulna Fracture may be sign with direct blow (Nightstick Fracture)
- Midshaft combined Radius and Ulna Fractures are typically high energy injuries (e.g. MVA, Sports Injury)
- Concurrent Soft Tissue Injury is common (as well as neurovascular injury)
VI. Types: Distal Forearm and Wrist Fractures
- See Distal Radius Fracture
- See Wrist Injury
-
Colles Fracture
- Distal Radius Fracture (often with ulnar styloid Fracture)
- "Dinner fork" deformity (distal fragment angulated dorsally)
-
Smith's Fracture
- Distal Radius Fracture with displacement towards volar aspect
- Opposite of Colles Fracture
- Children
- See Radial Epiphyseal Fracture
- Forearm Buckle Fracture (or Torus Fracture)
- Greenstick Forearm Fracture or complete Radius Fracture
VII. Types: Radius and Ulna Shaft Fractures
- Combined Ulna and Radius Mid-Shaft Fractures
- Typically require open reduction and internal fixation (ORIF)
- Risk of combined Fracture-dislocations (see GRUM below)
- Isolated Ulna mid-shaft Fracture
- Exclude associated Monteggia Fracture (see below)
- Mechanisms
- Fall (esp. going up stairs landing with Forearm against stairs)
- Direct blow (e.g. Nightstick Fracture)
- Mnemonic: GRUM (from distal radius to proximal ulna)

- GR: Galeazzi - Radius Fracture
- Distal Radius Fracture AND
- Lateral dislocation of the distal ulna injuring the Ulnar Nerve
- UM: Ulna Fracture - Monteggia
- Ulna shaft Fracture AND
- Displaced proximal radius, injuring the Radial Nerve (Wrist Drop)
-
Galeazzi Fracture
- Fracture of the distal shaft of radius
- Dislocation of Distal radio-ulnar joint (ulna will appear medially displaced at the wrist)
- Risk of Ulnar Nerve injury
-
Monteggia Fracture
- Proximal Ulna Fracture of shaft (typically displaced)
- Proximal Radial Head Dislocation
- Risk of Radial Nerve injury (e.g. thumb extension weakness)
{kind=link}
{kind=link}
VIII. Types: Proximal Forearm and Elbow Fractures
- Supracondylar Fracture of Humerus (most common in children)
-
Radial Head Fracture (most common in adults)
- Posterior arm splint for first 7 days
- Transition to sling use for total of 2-3 weeks
- Refer to orthopedics Mason 4, 3 (and possibly 2) Fractures
IX. Exam
- See Hand Neurovascular Exam
- See Elbow Exam
- Injury exam mantra: "joint above, joint below, circulation, motor function and Sensation, skin and compartments"
- Evaluate for Open Fracture
- Evaluate for Ecchymosis, deformity, shortening, rotation
- Evaluate wrist and elbow range of motion
- Evaluate elbow collateral ligaments with varus and valgus testing
X. Signs
- Localized Ecchymosis, swelling and tenderness at Fracture site
- Painful dorsiflexion has highest Test Sensitivity (>95%) for wrist Fracture
- Localized Ecchymosis has highest Test Specificity (>97%) for wrist Fracture
- Forearm may be shortened and displaced
- Pain may also be worse with wrist pronation
- Range of motion painful and diminished near the Fracture (elbow or wrist)
XI. Complications
- High rate of non-union in adults
- Risk of unstable Fractures even when initially non-displaced and despite external immobilization
- Radial Head Dislocation in proximal ulnar Fracture (Monteggia Fracture)
XII. Imaging
- Radius-Ulna Anteroposterior and Lateral XRay
- Should show entire Forearm including wrist and elbow
- Oblique XRay of elbow or Wrist
- Musculoskeletal Ultrasound of Forearm (Bedside Ultrasound, POCUS) has high accuracy in distal Forearm Fracture
- CT or MRI Elbow or Wrist
- Consider when other imaging is negative, but reduced range of motion (e.g. elbow extension)
XIII. Indications: Orthopedic Referral
- Orthopedic referral is indicated in most cases (aside from non-displaced or buckle Fractures)
- Allowable angulation and displacement is specific for each Fracture
- Distal Radius Fractures
- Combined Mid-Shaft Radial-Ulnar Fractures
- Most will require surgery and nearly all should be referred
- Fracture angulation, shortening, rotation or significant comminution
- Combined Fracture-Dislocations (Galeazzi Fracture or Monteggia Fracture)
- Isolated Ulnar mid-shaft Fractures
- Concurrent radius, wrist or Elbow Injury
- Significant comminution
- Proximal Ulna Fracture
- Fracture diaphysis displacement >50% bone diameter
- Fracture angulation >10 degrees
-
Radial Head Fracture
- Mason Type 4, 3 (and possibly 2) Fractures
XIV. Management: General
- Evaluate for Emergent Orthopedic Conditions
- Neurovascular Injury
- Open Fractures
- Compartment Syndrome
- Acute Fracture Management
- Acute Pain Management
- External Fracture reduction under Anesthesia as indicated
- Splint for 5-7 days, typically followed by Casting
- Orthopedic referral indications
- See above
XV. Management: Non-Mid-Shaft Fractures
- See Mid-shaft Radius-Ulna Fracture management as below
- See Distal Radius Fracture
- See Radial Head Fracture
- See Radial Epiphyseal Fracture
-
Forearm Buckle Fracture (children)
- Treated with short-arm splint, then Casting for total immobilization of 3 weeks
- Removable splint or nonrigid immobilization are reasonable alternatives
- Handoll (2018) Cochrane Database Syst Rev (12): CD012470 +PMID:30566764 [PubMed]
- Repeat Xray has been historically performed at 3 week follow-up visit
- However, some guidelines recommend follow-up imaging only for persistent symptoms or signs
- Riera-Alvarez (2019) J Pediatr Orthop B 28(6): 553-4 +PMID:32694434 [PubMed]
- Ling (2018) Radiol Res Pract +PMID:29686900 [PubMed]
- Treated with short-arm splint, then Casting for total immobilization of 3 weeks
-
Forearm Greenstick Fracture (children)
- Greenstick Fractures share the same treatment as complete non-displaced Radius Fractures
- Short-arm splint, then Casting for total immobilization of 3 weeks
- Allowable deformity without reduction (closed or ORIF) in age <10 years old
- Angulation <20-30 degrees (sagittal alignment, lateral XRay)
- Displacement <50%
- Greenstick Fractures share the same treatment as complete non-displaced Radius Fractures
-
Distal Radius Fracture (adults)
- See Distal Radius Fracture
- External Fracture reduction under Anesthesia as needed
- Splint with sugar-tong for first 5-7 days
- Transition to Short Arm Cast for 3-6 weeks
XVI. Management: Adults with Midshaft Radius-Ulna Fractures
- Displaced mid-shaft radius-Ulna Fractures
- May attempt closed reduction in emergency department under Anesthesia
- Sugar-Tong splint
- Orthopedic referral within 48 hours
- Open reduction and Internal Fixation (ORIF)
- Often indicated for displacement, shortening, angulation, rotation, comminution or instability
- Length of immobilization is shorter after ORIF as well
- Repeat Hand Neurovascular Exam before and after any manipulation or Splinting
- Non-displaced Midshaft radius-Ulna Fractures
- Initial long-arm Splinting for first 5-7 days
- Transition to Long Arm Cast with elbow at 90 degrees for 8-12 weeks
- Orthopedic referral if indicated as above
- Isolated Ulna Fracture
- Exclude Monteggia Fracture
- External Fracture reduction under Anesthesia as needed
- Splint with sugar-tong or posterior ulnar gutter for first 7-10 days
- Repeat XRay weekly for first 2-3 weeks
- Transition to Short Arm Cast or functional brace for 4-6 weeks
- Allowable deformity without surgery
- Fracture isolated to the ulna diaphysis middle or distal third
- Displacement <50% of bone diameter
- Angulation <10 degrees
XVII. Management: Children with Radius-Ulna Fractures
- Surgical intervention rarely needed
- Reduction Technique
- Anesthesia
- Angulated Fractures
- Traction and Counter traction
- Greenstick Fractures
- Often require breakage of opposite cortex
- Prevents re-angulation in cast
- Displaced Fractures
- Traction and Counter traction
- Slight bayonet apposition is acceptable
- Alignment must be satisfactory
- Immobilization in Long Arm Cast for 7-8 weeks
XVIII. Management: Follow-up
- Examine at weekly intervals for 3 weeks
- Inspect for re-angulation
- Angulation under 2 weeks
- Correct angulation manually
- Angulation over 2 weeks
- Angulation may be permanent
- Angulation under 2 weeks