
II. History
- History of injury
- Identify if risk of Retained Foreign Body (e.g. dirt, wood, glass)
- Identify contaminants (e.g. soiled knife)
- Concurrent serious injury (e.g. Closed Head Injury)
- Comorbid conditions
- Human Immunodeficiency Virus Infection or AIDS
- Diabetes Mellitus
- Other immunocompromising condition (e.g. Chemotherapy, chronic Corticosteroids)
- Medication allergies
- Latex Allergy
- Local Anesthesia allergy
- Tape allergy
- Antibiotic allergy
- Tetanus Immunization status
- Update with Td or Tdap if longer than 5-10 years since last Tetanus Vaccine
III. Exam
- Obtain adequate Hemostasis on presentation (e.g. direct pressure)
- See below for Hemostasis management
- See Hemorrhage Management
- See Topical Hemostatic Agent
- Identify functional loss prior to injecting Anesthesia
- Evaluate Muscle and tendon structures
- Evaluate nerve structures
- See Motor Exam
- See Sensory Exam
- Evaluate vascular structures
- Evaluate underlying bone
IV. Imaging
- Indications
- Fracture suspected
- Retained Foreign Body
- Modalities
V. Contraindications: Relative Contraindications to primary wound closure
- Infected and inflamed wounds
- Human Bite or Animal Bite
- Serious crush wounds
- Primary repair time constraints above not met
VI. Indications: Surgical Consultation
- Deep hand or Foot Wounds
- Full-thickness Eyelid or canniculus Laceration
- Consider for lip Lacerations, Ear Lacerations
- Nerve, artery, or bone involvement
- Traumatic Arthrotomy (joint involvement)
- Penetrating wounds of unknown depth
- Severe crush injuries
- Wounds requiring drainage (severely contaminated)
- Cosmetic outcome of significant issue
VII. Risk Factors: Wound Infection
- Age of Laceration Repair does not appear to significantly impact infection risk
- Diabetes Mellitus
- Laceration >5 cm
- Lower extremity Laceration
- Wound contamination
- Quinn (2014) Emerg Med J 31(2): 96-100 [PubMed]
VIII. Preparation: Closure Approaches
-
Wound Closure by Primary Intention (standard Laceration Repair)
- Immediate wound closure with Sutures, staples, surgical tape or Tissue Adhesive
-
Wound Closure by Secondary Intention
- Wound not closed, but rather allowed to heal naturally
- Typically used in badly contaminated wounds (e.g. Animal Bites, infected wounds)
- Delayed Primary Wound Closure (closure by tertiary intention)
- Delayed closure until after 3-5 days of observation for Wound Infection
- May also be considered in late wound presentations (>24 hours)
IX. Preparation: Closure Material
-
Suture Material
- See Suture Material for Suture type and size selection
- Deep (dermal or buried) Absorbable Sutures
- Vicryl is most commonly used for the deep layer, unless risk of infection (in which case use monofilament)
- Polyglecaprone 25 (Monocryl)
- Indicated for deep layer when wounds are higher risk of infection (Vicryl is contraindicated)
- Polydioxanone (PDS) is alternative to Polyglecaprone 25 (Monocryl) but has prolonged absorption
- Superficial Sutures (e.g. simple interrupted, RunningSuture)
- Nonabsorbable Sutures (standard approach)
- Absorbable Sutures (Controversial)
-
Tissue Adhesive
- See Tissue Adhesive
- Avoid use around the eyes due to risk of Cyanoacrylate Eye Injury and risk of Periorbital Cellulitis
- Limit to well-approximated, low tension, superficial Lacerations with linear edges
- Tape closure (Steri-strip) with Benzoin
- Remains attached for 4 days
- Lower risk of Wound Infection
- Place an extra steri-strip across each of strip ends
- Staples
- Indicated for Scalp Lacerations (tendons, nerves deep)
- Higher risk of infection when used for post-operative orthopedic and cesarean skin closures
X. Preparation: General
- Instrument pointers
- Use Adson's forceps ("pickups") with teeth (less crush injury)
- Grasp the needle driver (clamp) in palm of hand (without fingers in handle) for better control
- Use adson's forceps or similar (not fingers) to feed needle to needle driver
- Gloves
- Sterile gloves not needed in uncomplicated repair
- Perelman (2004) Ann Emerg Med 43:362-70 [PubMed]
- Ruler
- Estimates of length without a ruler are inaccurate (although women estimate better than men)
- Measurement is key if billing and coding are based on lesion length
- Peterson (2014) Injury 45(1): 232-6 [PubMed]
XI. Protocol: Repair timetable
- Age of Laceration does not appear to significantly impact infection risk
- Decision for primary closure should not solely be based on the age of Laceration ("golden period" for repair)
- Wounds involving nerves, blood vessels, tendons or bones have additional caveats
- Wounds <19 hours old heal better than those open for longer periods
- Bacterial count increase by 3 hours
- However Wound Infection risk is not directly correlated with age of Laceration
- See Risk Factors for infection as listed above
- Primary Repair
- See above precaution regarding no absolute cut-off for primary repair
- Face or Scalp: Repair within 24 hours (18 hours preferred)
- Body: Repair within 12-18 hours (6 hours preferred)
- Older wounds with infection risk
- Step 1: Initial Evaluation
- Option 1: Pack wound with sterile wet to dry dressings changed twice daily
- Option 2: Standard primary closure with simple interrupted Suture (no deep Sutures)
- Give precautions for immediate return for signs of infection
- Sutures are removed if wound becomes infected
- Option 3: Loose approximation with simple interrupted Suture (no deep Sutures)
- Loose closure is typically not recommended
- If choosing to Suture, close with good approximation (option 2)
- Lin and Vieth in Herbert (2018) 18(10):12-4
- Step 2: Reevaluation at 3-5 days
- No infection: Primary wound closure with Suture
- Infection: Treat infection and healing by second intention as below
- Alternative
- Step 1: Initial Evaluation
- Healing by second intention
- Pack wounds with sterile wet to dry dressing bid
- Granulation and Contraction risk without suturing
XII. Protocol: Local Anesthesia
- See Local Skin Anesthesia (includes pearls to decrease patient discomfort)
- Prepare skin with antiseptic prior to injection
- Consider Topical Anesthetics, especially in children (e.g. LET Anesthesia)
-
Epinephrine is safe in areas previously contraindicated (fingers, toes, ears, nose)
- Exercise caution in Peripheral Vascular Disease
- Digits (even Digital Block): 1:100,000 Epinephrine concentration
- Nose/Ears: 1:200,000 Epinephrine concentration
XIII. Protocol: Irrigation
-
Personal Protection Equipment
- Wear a mask with eye shield during irrigation
- Saline is as effective as antiseptics (e.g. 1% Betadine) for irrigation
- Antseptics should be avoided inside the wound due to tissue injury
- Tap water is as safe and effective as saline for irrigation (and more plentiful)
- Moderate pressure irrigation is the key
- Irrigation with syringe provides approximately 5-8 psi
- Irrigate with minimum of 250 to 500 cc, or 50-100 ml/cm wound length (use 1000 cc or more if contaminated)
- Normal Saline irrigation, compressible plastic bottles (250-500 cc) with plastic adapter OR
- Syringe 30-60 ml syringe (requires multiple refills) OR
- Placing wound under Running tap water
- Avoid irrigation with tissue destructive agents
- Hydrogen Peroxide (weak germacide)
- Betadine at stock concentration (9%)
- Always dilute Betadine (1:10)
XIV. Protocol: Wound Preparation
- Remove all surface foreign bodies with scrub brush on skin surface
- Do not apply Betadine or Hibiclens inside of wound
- Apply to wound edges prior to Anesthesia injection (see Local Anesthesia as above)
- Drape widely to allow clear margins
-
Scalp Wounds
- Slick surrounding hair down with K-Y Jelly
- Lacerations near the eye
- See Eyelid Laceration
- Avoid Tissue Adhesive if possible (risk of Cyanoacrylate Eye Injury and increased risk of Periorbital Cellulitis)
- Do not shave eyebrows
-
Thin Skin Flaps (Skin Tears, especially in elderly)
- See Skin Tear
-
Facial Nerve region
- Exercise caution in region of Facial Nerve, especially near Parotid Gland and mandubular branch
- Risk of permanent nerve injury
- Prevent excessive swelling that may compress Facial Nerve branches (consider wound drains)
XV. Management: Hemostasis
- See Tourniquet (Pneumatic Tourniquet, Windlass Tourniquet)
- See Topical Hemostatic Agent
- See Hemorrhage Management
- Precautions
- Patient reports of spurting or pumping bleeding is arterial injury until proven otherwise
- Arterial injury may not be immediately obvious on Emergency Department presentation
- Arterial bleeding may stop briefly due to vasospasm and small thrombus formation
- Do not ligate named arteries
- Consult surgery if arterial injury is suspected
- Management of small artery bleeding
- Apply direct pressure
- Arteries <2mm
- Locally infiltrate Lidocaine with Epinephrine
- Consider electrocautery
- Small, unnamed arteries >2mm
- Ligation (if able to identify the bleeding vessel)
- Clamp the bleeding end and apply ligature (Suture)
- Figure of eight Suture (or horizontal mattress)
- Indicated for vessel that has retracted within tissue and cannot be clamped
- Imagine a square box around the bleeding source
- Each corner of the exposed square represents an entry or exit of the figure of eight Suture
- Tying the figure of eight compresses the tissue around the bleeding source
- Ligation (if able to identify the bleeding vessel)
XVI. Protocol: Wound Repair
- Specific injury approaches
- See Finger Laceration
- See Scalp Repair
- See Wound Dressing for Transport
- Indicated if repair must be done elsewhere
- Lip Laceration
- Reapproximation of vermillion border is critical to optimal cosmetic result
- Place first Suture to reapproximate vermillion border
- Use skin marker at border before Anesthetic injection
- Repair deeper Muscle and Oral Mucosa with 4-0 Absorbable Suture
- Repair skin with 6-0 nylon (e.g. Ethilon)
- Deep injuries with full thickness muscle Lacerations
- Muscle does not hold Sutures well
- Attempt to close Muscle with 2-0 or 3-0 Absorbable Suture, using Horizontal Mattress Suture
- Consider closing fascia above and below Muscle
- Lin, Shinar and Kantor in Herbert (2017) EM:Rap 17(8): 1-2
-
Debridement
- Recut wound for clean, fresh, surgical-incision edges
- Undermining
- May be required to ensure Dermis closure and decreased skin tension
- Best dissection plane is between dermal layer and connective tissue, subcutaneous fat
- Insert closed scissors on lateral wound margin, and then spread open
- Repeat for opposite lateral wound margin
-
Suture technique
- General pearls
- Grasp Suture Needle with needle driver one third of way from Suture attachment (where needle becomes straight)
- Tie the knot with two square knots (4 ties, or for narrow Suture use 5 to 6 ties)
- The first knot should have 2 loops or throws around the needle driver to "set" the knot
- Cut Suture to 3-5 mm length
- Evert wound edges (do not dig a ditch, build a flask)
- Everted edges will flatten over time, inverted edges result in more prominent scars
- Needle should enter perpendicular to skin
- Direct the needle initially down and away from the Laceration edge
- Rotate the wrist and needle driver, following the needle curvature
- Exit perpendicular to the skin surface on the opposite side of the Laceration
- Reduce skin tension
- High skin tension results in a wound that may gape open with risk of Hypertrophic Scar
- Avoid tying knots too close to the wound (increases skin tension)
- Wound eversion is a good sign that skin tension has been reduced across the wound edge
- Avoid subcuticular closure as sole repair method
- Techniques to reduce skin tension
- Use deep Sutures first, before superficial closure
- Undermine skin edges
- In contaminated wounds use simple interrupted Suture or Vertical Mattress Suture
- Interrupted simple mnemonic
- Not too many
- Not too tight
- Not too wide
- Get them out
- References
- Lin, Kantor and Shinar in Herbert (2017) EM:Rap 17(4): 1
- General pearls
- Techniques
- See Wound Closure with Staples
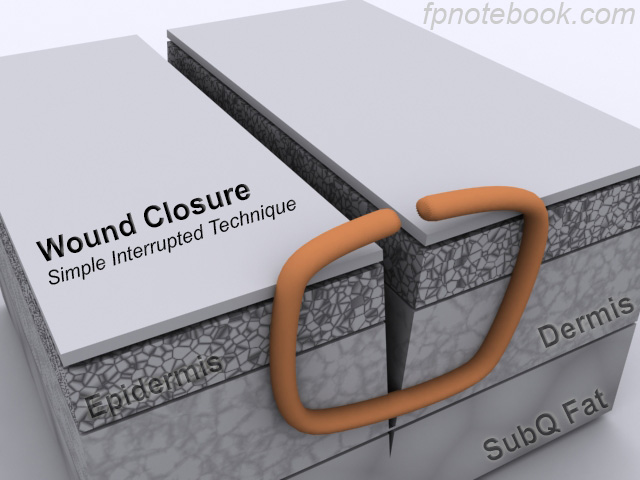
- Simple Interrupted Suture
- Work-horse of Laceration Repair (appropriate for nearly all repairs)

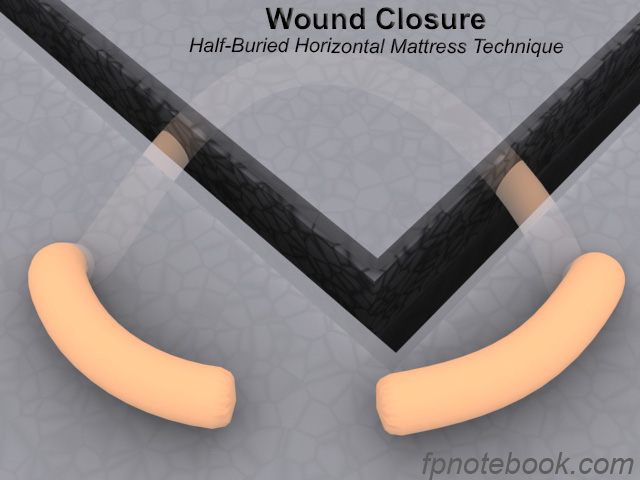
- Half-buried Horizontal Mattress Suture
- Indicated in triangular flap Laceration (does not compromise blood supply to tip of corner)

- Horizontal Mattress Suture
- Everts wound edges, but risk of skin necrosis and scar

- Vertical Mattress Suture
- Everts wound edges, but risk of skin necrosis and scar

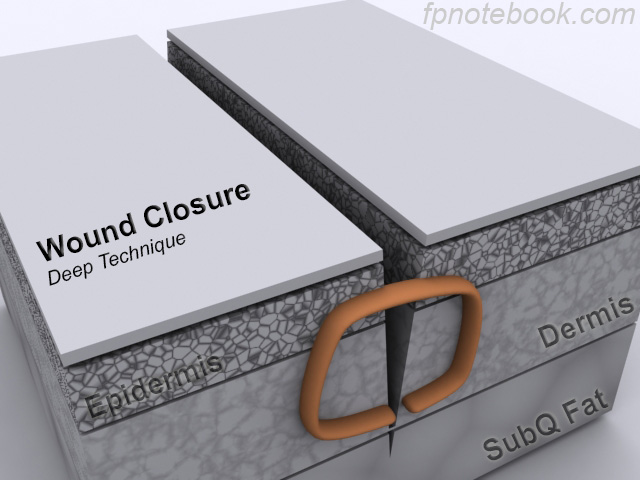
- Deep Suture (interrupted dermal Sutures)
- May use in clean wounds to better approximate wound edges and reduce wound edge tension

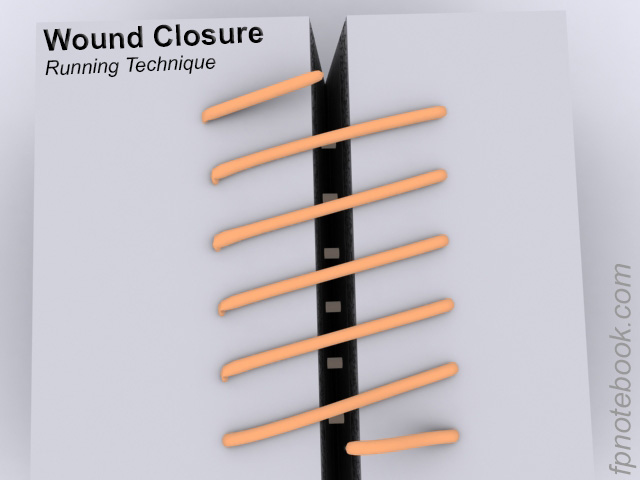
- RunningSuture
- Fast technique for long Lacerations, but risk of dehiscence if Suture breaks anywhere along its length

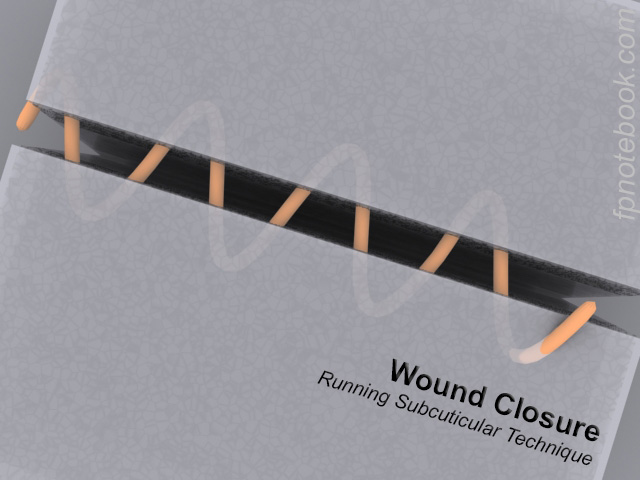
- Running Subcuticular Suture
- May use in clean wounds (surgical wounds) for close wound edge apposition (but does not allow drainage)

- Suture Removal


XVII. Protocol: Bandages
- Moist Wound Healing is key
- Non-adherent slightly moist or Occlusive Dressing
- Ointment or Topicals (e.g. Bacitracin, vaseline)
- Apply for first 3 days until epithelialization
- Reduces infection risk at minor wound sites
- Precautions
- Avoid applying ointment over Skin Glue closure (e.g. Dermabond)
- Vaseline alone is sufficient without risk of reaction and without higher rate of Wound Infections
- Topical Antibiotics cause a irritant or Allergic Contact Dermatitis in up to 10% of cases
- Reactions are most common with neosporin (or triple antibiotic)
- Reactions may also occur with Bacitracin
- Consider Debridement after epitheliazation (day 3)
- Initial use of Occlusive Dressings (first 3 days) prevent scab formation
- Carefully apply 50% Hydrogen Peroxide to scab
- Avoid prior to day 3 (delays Wound Healing)
- Scab removal may improve cosmesis
XVIII. Protocol: Home Instructions
- Gentle compression
- Precautions about water exposure (e.g. bathing, getting wound wet)
- Typical recommendations are to not get the wound wet for the first 48 hours after repair
- Early water exposure at a wound site does not appear to increase the risk of infection
- Patients should still avoid exposure to contaminated water (e.g. dish washing)
- Observe and return immediately for signs of Wound Infection
- Avoid excessive tension on wound edges (risk of wound dehiscence)
-
Suture Removal
- See Suture Removal Timing
- Face, Ear, Eyebrow, Nose, Lip: 5 days (3 days for Eyelid)
- Other regions: 10 days
- Scar prevention
- See moist Wound Healing recommendations as above
- After Wound Healing (first 28 days), consider Silicone Sheeting applied daily for up to 3 months
XIX. Management: Adjuncts
- Prophylactic antibiotics possible indications
- Not routinely indicated in noncontaminated wounds
- Wounds at higher risk of secondary infection
- See secondary infection risk factors below
- Comorbidity with risk of distant site infection
- Endocarditis risk (see SBE Prophylaxis)
- Hip prosthesis
- Post-exposure Tetanus Prophylaxis
- Unknown Immune Status or never immunized
- Tetanus Toxoid Containing Vaccine (e.g. Td, Tdap, TT) now, at 6 weeks and 6 months AND
- Tetanus Immune globulin 250 Units IM if Puncture Wound or contaminated wound
- Last Tetanus Toxoid containing Vaccine over 5-10 years prior
- Tetanus Toxoid Containing Vaccine (e.g. Td, Tdap, TT) now
- Unknown Immune Status or never immunized
XX. Management: Disposition
- Hospitalization Indications
- Failed outpatient therapy (especially if non-compliance with recommended management)
- Poorly controlled comorbidity (e.g. Diabetes Mellitus, Peripheral Vascular Disease)
- Immunocompromised state
- Severe or progressive Cellulitis (especially if deeper, regional or systemic signs)
- Necrotizing Fasciitis
- Referral or Consultation Indications
- Wounds affecting joints, bones, tendons or nerves
- Wounds affecting large body regions
- Facial wounds
- Burn Injury
- See Burn Injury for referral/transfer criteria
- Severe or circumferential burns or
- Burns to the face, hands or feet
XXI. Complications
- Retained Foreign Body
- Hypertrophic Scar
- Secondary Wound Infection
- See Wound Infection for risk factors
- Occurs within 48 hours in most cases
XXII. Course: Wound Healing
- See Wound
XXIII. References
- Lin and Lin in Herbert (2014) EM:Rap 14(11): 8-10
- Lin and Mason in Herbert (2022) EM:Rap 22(6): 12-14
- Lin and Shinar in Herbert (2017) EM:Rap 17(5): 3-4
- Lin and Shinar in Herbert (2017) EM:Rap 17(7): 1-2
- Mortiere (1996) Principles of Primary Wound Management
- Snell in Pfenninger and Fowler (1994) Procedures for Primary Care Physicians, Mosby, Chicago, p. 12-9
- Forsch (2017) Am Fam Physician 95(10): 628-36 [PubMed]
- Worster (2015) Am Fam Physician 91(2): 86-92 [PubMed]