
II. Epidemiology
- Most common Partial Cord Syndrome
III. Pathophysiology
- Hyperextension of the Cervical Spine (e.g. fall onto face)
-
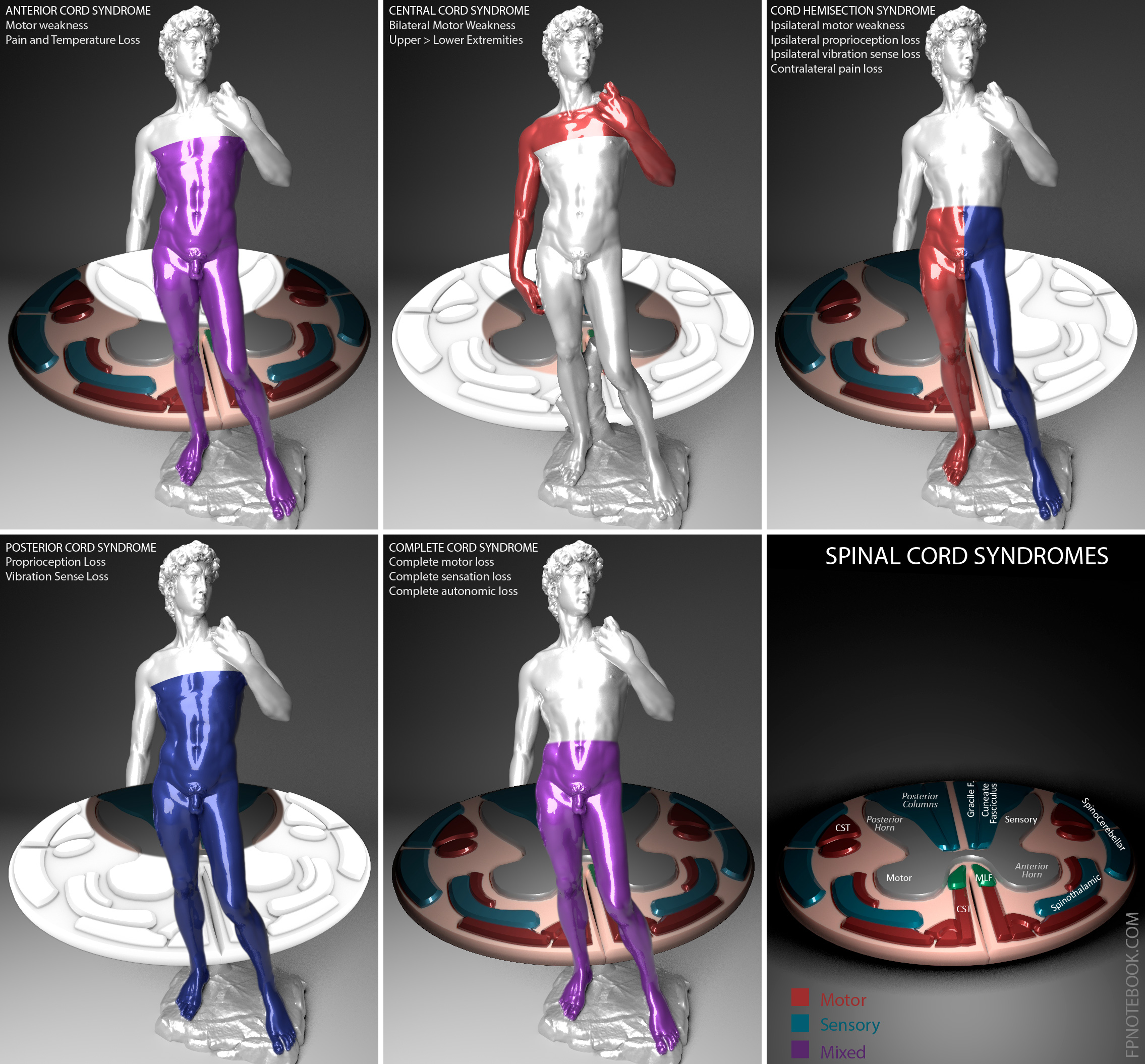
Edema and Hemorrhage into the central cord
- Gray matter
- Spinothalamic Tract (pain and Temperature sense) may be affected
- Spinothalamic Tract injury is more associated with Anterior Cord Syndrome
- Lateral Corticospinal tracts (motor function)
- Upper extremities are localized to the medial or central aspect of the Corticospinal tract
- Upper extremities are more affected than lower extremties in Central Cord Syndrome
- Images
IV. Precautions
- Have a high index of suspicion in Trauma
- Findings may initially be subtle and mistakenly attributed to peripheral injury
V. Causes
- Older patients (most common)
- Athletes
- Hyperextension with ligamentum flavum buckling
- Other mechanisms
- Unrestrained in Motor Vehicle Accident
VI. Signs
- Bilateral motor weakness
- Upper extremities affected more than the lower extremities
- Distal extremities affected more than proximal extremities
- Sensory deficiency
- Variable
- Hyperesthesia may be present
VII. Imaging
VIII. Management
- See Trauma Evaluation
-
General Measures
- Full Spine Immobilization
- Maintain mean arterial pressure 85 to 90 mmHg
- Preserve injured cord perfusion and prenumbra
- Corticosteroids are NOT recommended (since 2013 in U.S.)
- Despite associated inflammatory cascade and associated compression
- Consult Neurosurgery
- Decompression Surgery
- In acute Trauma-related cases, may result in better neurologic outcomes
- Anderson (2015) Neurosurgery 77(suupl 4):S15-32 [PubMed]
IX. Prognosis
- Better than with other Partial Cord Syndromes
X. References
- Broder (2022) Crit Dec Emerg Med 36(3): 25
- Decker in Chorley and Bachur (2014) Overview of Cervical Spinal Cord Injuries..., UpToDate, Wolters-Kluwer
- Rodriguez, Winger, Poulo and Glunk (2023) Crit Dec Emerg Med 37(3): 23-9
- Wagner (1997) Emerg Med Clin North Am 15:699-711 [PubMed]