
II. Indications
- Airway Protection
- Unconscious patient (Glasgow Coma Scale <=8) or significantly altered
- Intracranial Hemorrhage
- Severe Closed Head Injury
- Status Epilepticus
- Drug Overdose with CNS depression
- Multiple Trauma, Head Injury, abnormal mental status or severe, refractory Agitation
- Other aspiration risk
- Bleeding into upper airway
- Vomiting
- Unable to speak or swallow
- Airway obstruction risk
- Anaphylaxis or Angioedema
- Neck Mass or Stridor
- Mouth or neck infection
- Severe Maxillofacial Trauma
- Inhalation burn or other Inhalation Injury (with cord edema)
- Neck Hematoma
- Tracheal injury
- Neck foreign body
- Unconscious patient (Glasgow Coma Scale <=8) or significantly altered
- Ventilation and Oxygenation
- Respiratory arrest
- Respiratory Failure (e.g. Asthma, COPD, Pneumonia, Pulmonary Edema)
- Hypoventilation/Hypercarbia
- paCO2 >55 mmHg
- Arterial Hypoxemia refractory to oxygen
- paO2 <55 RA, <70 on 100% Face Mask
- Respiratory Acidosis
- Hypoventilation/Hypercarbia
- Need for prolonged Ventilatory support
- Class III or IV Hemorrhage with poor perfusion
- Sepsis or other severe Metabolic Acidosis
- Severe Chest Injury (e.g. Flail Chest or Pulmonary Contusion)
- Neuromuscular disorder (e.g. Guillain Barre, Myasthenia Gravis)
- Vital Capacity <20 ml/kg predicts high risk of Respiratory Failure (indicates ICU monitoring)
- Intubation based on clinical findings (e.g. Tachypnea, discomfort)
- References
- Strayer (2017) EM:Rap 18(8): 9-10
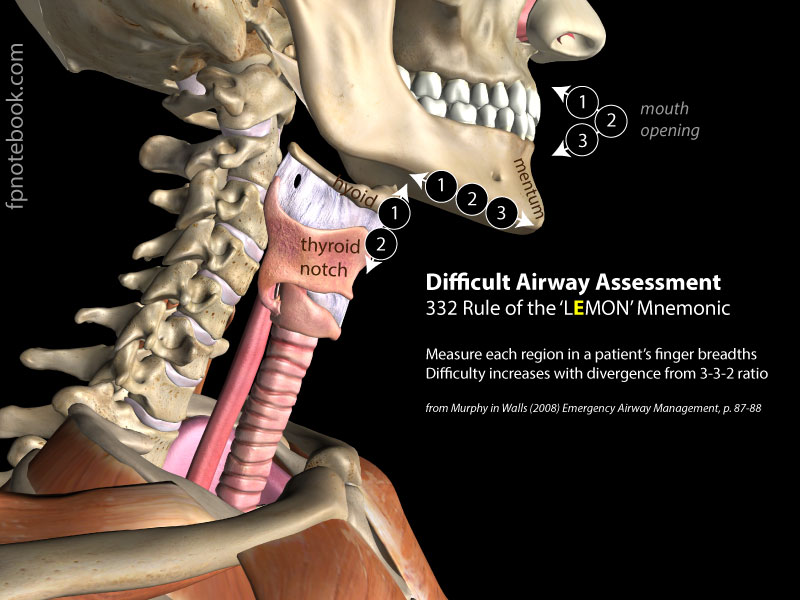
III. Assessment (from the Difficult Airway Course)
- Anticipate difficult Direct Laryngoscopy (Mnemonic: LEMON)
- Look externally (gestalt)
- Evaluate the 3-3-2 rule
- Significantly more or less than these values suggests more difficult airway management
- Measure each of 3 parameters using patient's own finger breadths
- Three fingers of mouth opening
- Three fingers between mentum and hyoid
- Two fingers between hyoid and Thyroid cartilage
- Images
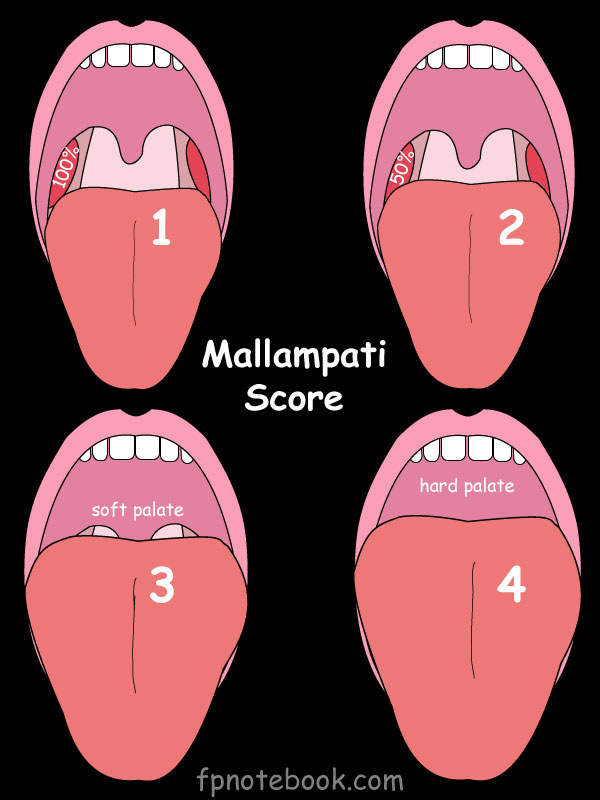
- Mallampati Score
- Score of 3-4 suggests higher risk
- Images
- Obstruction ("hot potato voice", inability to swallow secretions, Stridor)
- Severe Angioedema
- Supraglottic swelling
- Smoke Inhalation
- Neck mobility reduced (e.g. Cervical Spine Immobilization, Rheumatoid Arthritis)
- Anticipate difficult mask ventilation (Mnemonic: MOANS)
- Mask seal (e.g. beard)
- Obstruction
- Older Age
- No teeth (replace dentures for Bag Valve Mask Ventilation)
- Stiff lungs requiring increased Ventilatory pressures (Asthma, COPD, ARDS, term pregnancy)
- Anticipate difficult Cricothyrotomy (Mnemonic: SHORT)
- Anticipate difficult Extraglottic Device (Mnemonic: RODS)
- Restricted mouth opening
- Obstruction of the upper airway or Larynx
- Distorted or disrupted airway
- Stiff lungs requiring increased Ventilatory pressures (Asthma, COPD, ARDS, term pregnancy)
- References
- Reed (2005) Emerg Med J 22:99-102 [PubMed]
- Difficult Airway Course
IV. Precautions: Aspiration Risks (avoiding Vomiting during intubation is critical)
- Full Stomach (4-6 hours from last meal)
- Head Trauma (ICP increase, swallowed blood)
- Delayed Gastric Emptying
- Intestinal Obstruction
- Obesity
- Pregnancy
V. Protocol: Overview
- See Emergency Decision Cycle (OODA Loop, AAADA Model)
- Airway management always begins by opening the airway (e.g. position the head and neck)
- Advanced Airway is indicated (based on above indications)
- Equipment: Laryngoscope
- Video Laryngoscopy is superior to Direct Laryngoscopy for successful intubation (by Odds Ratio >12)
- Sakles (2012) Ann Emerg Med 60(6):739-48
- However, Direct Laryngoscopy is most common means of rescuing Video Laryngoscopy (e.g. Glidescope) failure
- Best to maintain Direct Laryngoscopy skills to use as back-up procedure for device failure or malfunction
- Levitan and Brode in Majoewsky (2013) EM:Rap 13(1): 10
- Video Laryngoscopy is superior to Direct Laryngoscopy for successful intubation (by Odds Ratio >12)
- Consider which of the 3 approaches is indicated
- Crash Airway (patient comatose or in cardiopulmonary arrest)
- Able to ventilate
- Attempt intubation
- If initial attempt fails, give Succinylcholine 2 mg/kg IV
- Make up to 3 additional attempts at intubation
- Unable to ventilate or oxygenate
- Go below to failed airway
- Able to ventilate
- Difficult airway expected
- Call for help
- Unable to oxygenate or ventilate with Bag Valve Mask prior to any intervention attempt
- Consider BIPAP or CPAP for preoxygenation
- Prepare for Cricothyrotomy (see failed airway below)
- Consider Scott Weingart's CriCon double set-up approach
- Rapid Sequence Intubation with a single intubation attempt
- Consider Elastic Bougie placement, BIPAP, and then Endotracheal Tube placed over bougie
- Go below to failed airway
- Able to ventilate (with Bag Valve Mask)?
- Yes: May precede below with Rapid Sequence Intubation
- No: Anticipate inability to effectively Bag Valve Mask (PPV)
- Use awake patient measures
- Visualize airway under Local Anesthetic
- Direct Laryngoscopy or Video intubation
- Consider placing Elastic Bougie if cords visualized
- Fiberoptic intubation (e.g. flexible bronchoscopy)
- Light sedation and Local Anesthetic (e.g. cetacaine spray)
- Consider drying agent (e.g. glycopyrolate)
- Thread endoscope through ET Tube lumen and insert scope via nose or mouth
- Rapid Sequence Intubation (routine intubation allows time for premedication)
- Crash Airway (patient comatose or in cardiopulmonary arrest)
- Failed airway options
- Failed intubation or cervical immobilization?
- Elastic Bougie guided intubation
- Tactile Orotracheal Intubation (Digital Intubation)
- Laryngeal Mask Airway (or other extraglottic airway) to temporize
- Nasotracheal Intubation (if no Maxillofacial Trauma, Basilar Skull Fracture)
- Intubating Laryngeal Mask Airway (intubating LMA)
- Cannot intubate, cannot oxygenate (and cannot ventilate): CICO
- Cricothyrotomy ("cut to air")
- Failed intubation or cervical immobilization?
VI. Resources
- FPnotebook: Virtually Resuscitated RSI
- Airway Cam (Levitan)
- Airway World (Walls, requires free registration to view videos)
VII. References
- Majoewsky (2012) EM: RAP-C3 2(5): 3-4
- Levitan (2013) Practical Airway Management Course, Baltimore
- Walls (2012) Emergency Airway Management, 3rd Ed, Lippincott, Philadelphia, p. 9-22, 82-93
- Fuchs and Yamamoto (2011) APLS, Jones and Bartlett, Burlington, p. 40-1