
II. Physiology
- Innervates extraocular Muscle: Superior Oblique Muscle
- Superior Oblique Muscle passes via pulley (trochlea)
- Long thin nerve that is susceptible to compression (Cranial Nerve 4 and 6 are similar in this way)
- Paralysis (unilateral or bilateral) may occur even with generalized Increased Intracranial Pressure
- Contrast with the Cranial Nerve 3
III. Anatomy
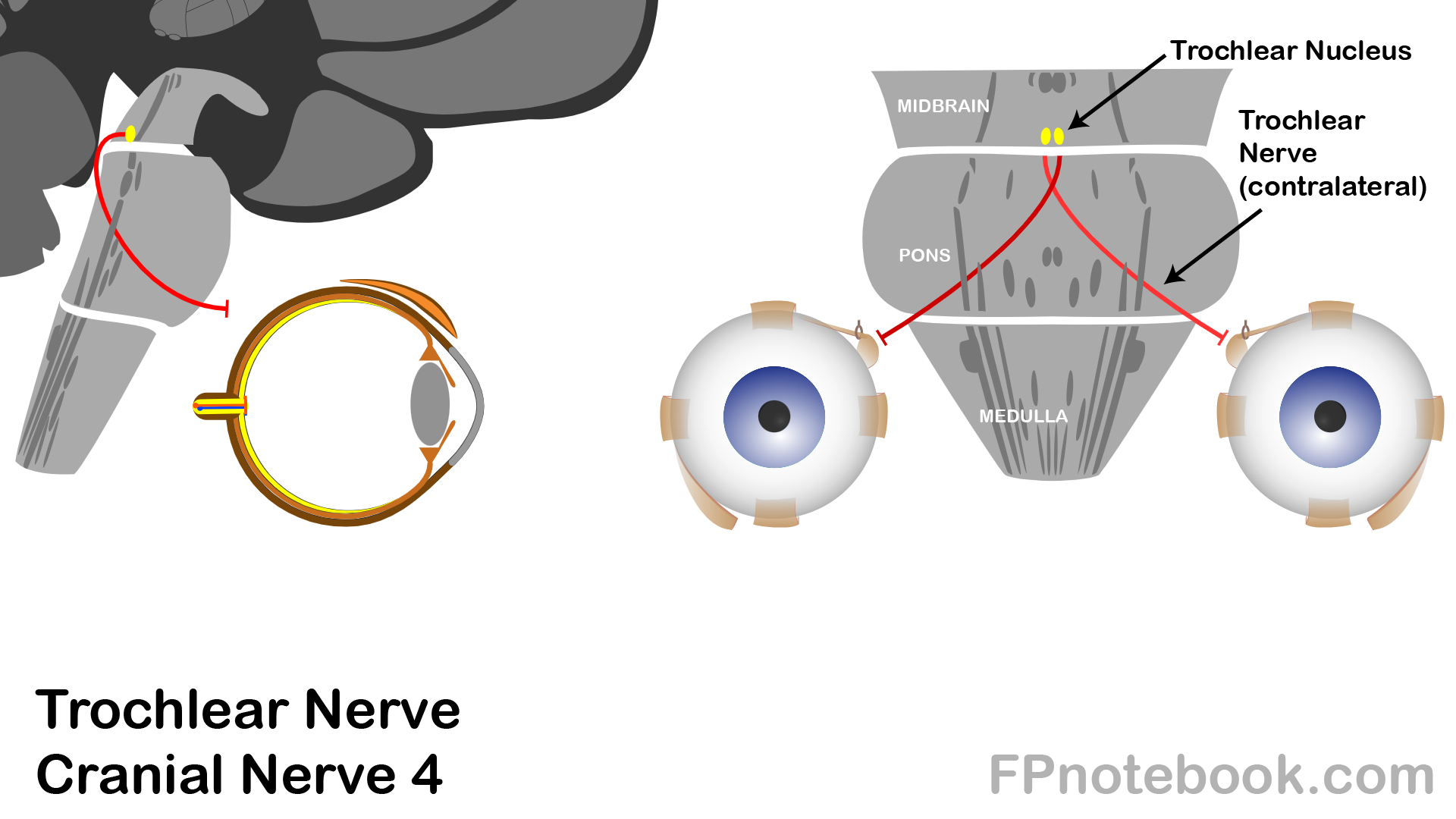
- Nucleus
- Trochlear Nucleus is at the floor of Cerebral Aqueduct in the Midbrain
- Unlike all other Cranial Nerves:
- CN 4 crosses the midline, innervating the contralateral side (all other Cranial Nerves are ipsilateral)
- CN 4 exits posteriorly (all other Cranial Nerves exit anterior to the Brain Stem)
- Course
- Tracks around superior cerebellar, cerebral peduncles
- Enters tentorium cerebelli at posterior clinoid process
- Proceeds through lateral wall of Cavernous Sinus
- Enters orbit via superior orbital fissure
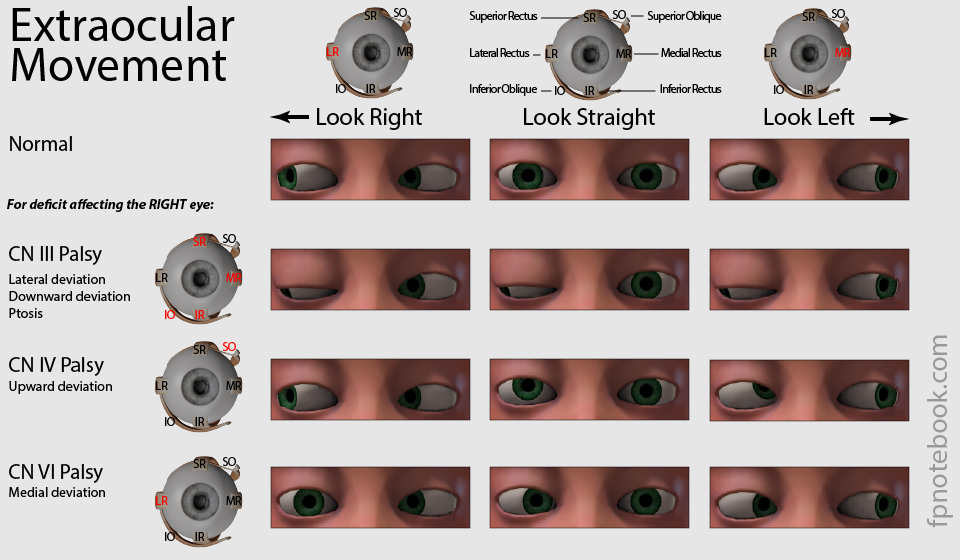
IV. Exam
- Extraocular Movement
- Normal function of the Superior Oblique Muscle
- Eye movement inferior laterally
- Paralysis of the Superior Oblique Muscle
V. Causes: Cranial Nerve 4 Palsy
- Congenital Palsy
- Head position changes may occur to compensate for Strabismus and Diplopia
-
Trauma
- Longest nerve course with higher risk of injury
- Increased Intracranial Pressure may also cause palsy (as nerve is relatively thin)
- MIcrovascular (small vessel disease)
- More common in older patients with Cardiovascular Risk Factors (e.g. Diabetes Mellitus)
VI. References
- Gilman (1989) Manter and Gatz Essentials of Neuroanatomy and Neurophysiology, Davis, p. 87-113
- Goldberg (2014) Clinical Neuroanatomy, p. 24-39
- Netter (1997) Atlas Human Anatomy, ICON Learning, p. 110-129