
II. Indications
- Tension Pneumothorax (following immediate Needle Decompression of Thorax)
- Simple Pneumothorax
- Open Pneumothorax
- Massive Hemothorax
- Penetrating Chest Trauma
III. Contraindications: Relative
- Underlying pleural adhesions
- Underlying Emphysematous blebs
- Coagulopathy
IV. Precautions
-
Tension Pneumothorax requires immediate Needle Decompression of Thorax
- Chest Tube placement is only after the Needle Decompression of Thorax has been completed
- Indications for operative management in Traumatic hemothorax
- Chest Tube output >1500-2000 cc total or
- Chest Tube output 150-200 cc/hour for several hours
- Do not choose an insertion site too low
- Ideal insertion site is at the 4th or 5th intercostal space (mid or anterior axillary line)
- Err on the side of higher instead of lower
- Diaphragm reaches the 7th intercostal space on expiration
- Peritoneal Chest Tube placement occurs in 1% of cases
- Emergency department doctors were below the 5th intercostal space in 64% of cases
- Below the 7th intercostal space 21% of cases (below the 8th in 9% of cases)
- Placement was more accurate in women than men
- British Thoracic Society recommends staying within the "triangle of safety", with apex at axilla
- References
- Arora and Menchine in Herbert (2015) EM:Rap 15(2): 13
- Carter (2014) Emerg Med Australas 26(5): 450-4 +PMID:25212066 [PubMed]
- Ideal insertion site is at the 4th or 5th intercostal space (mid or anterior axillary line)
V. Preparation: Equipment
- Tube size
- French tube size is diameter of tube in millimeters multiplied by 3 (e.g. 36 French = 12 mm diameter)
- Spontaneous uncomplicated Pneumothorax: 16 to 22 French (small bore)
- Unstable Patient, Bronchopleural Fistula or Mechanical Ventilation: 24 to 28 French
- Complicated Pneumothorax or Hemothorax (Trauma): 28 to 32 French (large bore)
- Older recommendations were for 36-40 French Chest Tube in Hemothorax
- Recent evidence supports smaller Chest Tubes even for Hemothorax (28 French is most common)
- Similar complication rates (e.g. empyemea, retained Hemothorax) regardless of tube size
- Inaba (2012) J Trauma Acute Care Surg 72(2): 422-7 [PubMed]
- Chest Tube Suction Apparatus or pleur-evac
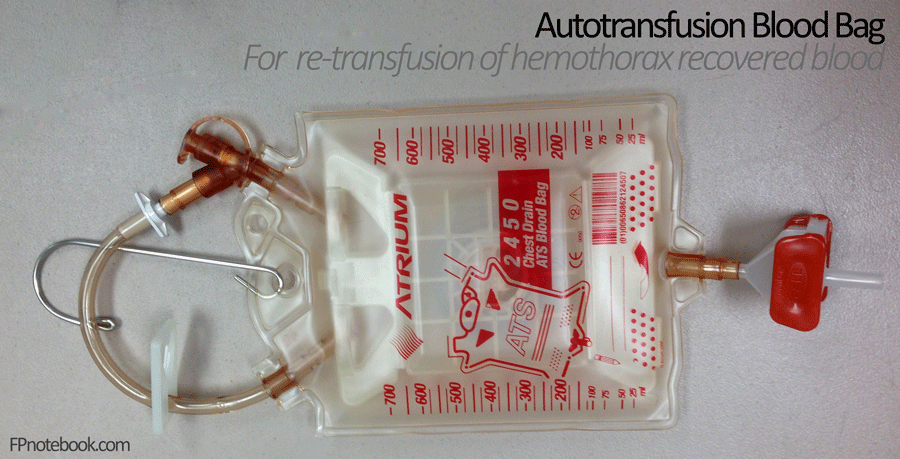
- Cell salvage device (Autotransfusion blood bag, cell-saver) for Hemothorax blood recovery

- Filtered blood (and treated with citrate phosphate dextrose)
- Contraindicated if pleural contamination, thoracic infection or malignancy, DIC, Sickle Cell Anemia
- Minimum volume of Hemothorax collection is 700 ml
- Blood may be re-transfused in Massive Hemothorax for up to 6 hours after collection (prefer <4 hours)
- Spares utilization of allogenic blood and Platelet Transfusion
- Replaces blood cells, Platelets and Fresh Frozen Plasma (FFP)
- Hemoglobin is less concentrated than packed RBC (9 g/dl compared with 13 g/dl in pRBC)
- Inadequately filtered blood may introduce Leukocytes, Cytokines, small particular aggregates
- Similar safety to allogenic transfusion
- References
VI. Preparation
- Personal Protection Equipment
- Povidone Iodine (Betadine) or Chlorhexidine (Hibiclens) prep and drape a wide area
- Expose surrounding landmarks (axilla, clavicle, Sternum, costal margin)
-
Anesthetic
- Lidocaine 1% with epinephrine Local Anesthetic to skin and down to rib (fan injection)
- Chest Tube
- Clamp 1: Holds insertion end of Chest Tube
- Clamp 2: Clamps off the other end of tube, so chest contents does not spill from tube
- Optimize procedure conditions (esp. in obese patients, in whom landmarks are difficult)
- Adequate lighting
- Leave a wide prepped area free of draping to allow visualization of landmarks (chest, axilla)
- Use a longer incision in obese patients
- Consider Procedural Sedation (e.g. Ketamine)
- Patient positioning
- References
- Spangler and Inaba in Herbert (2016) EM:Rap 16(9): 7
VII. Technique
- Image
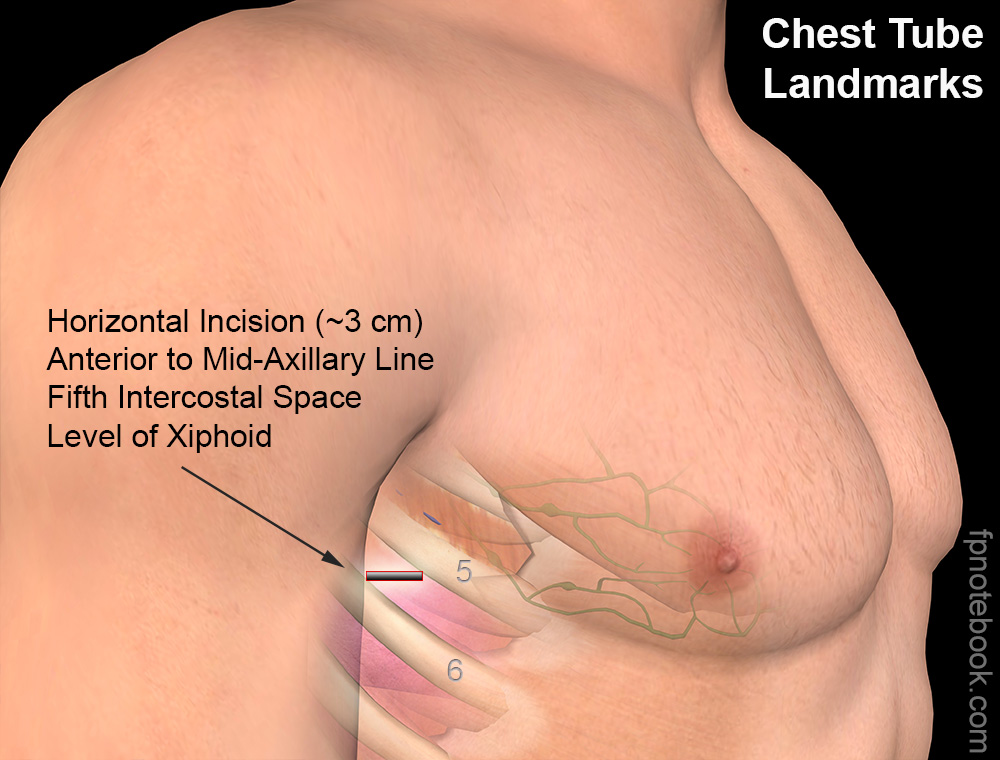
- Insertion Site
- See precautions above
- Insert anterior to mid-axillary line
- Level of 5th intercostal space, over 6th rib
- Men: Nipple line
- Women: Xiphoid process level or inframammary fold
- Triangle of safety
- Insertion length or tube
- Estimate distance from the 6th intercostal space to the Shoulder
- Note the marker position on the Chest Tube that covers that distance (deepest insertion point)
- Last hole on Chest Tube must be in chest or it will need to be replaced
- Tube distance marks are measured from the last hole position to the tip
- Insertion Procedure
- Incise horizontally 3 cm parallel and over the top of the 6th rib (incision should follow the course of the rib)
- Consider a wider incision in patients with a larger chest wall (to ensure successful placement)
- Consider injecting additional Local Anesthetic into the subcutaneous tissue above the intended rib entry site
- Bluntly dissect through subcutaneous tissue over rib with clamp
- Carefully puncture parietal pleura with clamp tip
- Firmly grasp Chest Tube several centimeters from insertion site
- Hand acts as a stopper
- Prevents clamp from being forced too deep on puncture of the pleural space
- Insert finger into incision and make 360 degree sweep
- Check for organs, adhesions and enlarge path
- Insert Chest Tube tip with clamp
- Once the pleura is opened, any potential emergency related to Tension Pneumothorax is resolved
- The tube insertion can be delayed if the provider needs to return to airway management
- Take time to ensure the Chest Tube is properly inserted
- Firmly grasp tube and hold in place while withdrawing clamp
- Finger adjacent to the tube can confirm the Chest Tube direction is toward the apex
- Insert at least 12 cm to ensure all Chest Tube holes are in chest
- May need to insert 16 cm or more in very large patients
- Smaller patients may only allow 10 cm of insertion
- Insertion direction
- The tube typically can not be directed once it leaves the clamp
- Ideally, direct toward apex for for Pneumothorax, posterior-laterally for Hemothorax
- Avoid inserting toward hilum or mediastinum
- Once the pleura is opened, any potential emergency related to Tension Pneumothorax is resolved
- Clinical signs of proper tube placement
- Look for tube condensation indicating good placement (unclamp proximal tube end)
- Rotate tube - should turn freely if not kinked
- Incise horizontally 3 cm parallel and over the top of the 6th rib (incision should follow the course of the rib)
- Procedure Completion
- Close skin around the Chest Tube entry
- Suture tube in place (0 or 1 non-Absorbable Suture, e.g. silk ties)
- Cover tube entry with petroleum-impregnated gauze
- Tape tube in place (Rubber tape)
- Attach Chest Tube to suction
- Underwater seal apparatus and suction (-20 to 30 cm H2O)
- Pleur-evac
- Chest XRay
- Verify position and function of tube
- Suction
- Keep Chest Tube clamped until suction applied
- Can place to passive water seal initially
- Suction can be delayed initially in most cases to allow for securing the tube
- Exceptions include a large Bronchopleural Fistula which requires immediate suction
- Hemothorax will often drain without wall suction (blood is forced out with respirations)
- See Hemothorax
- See Autotransfusion protocol in Massive Hemothorax (esp. >2000 ml)
- Pneumothorax requires suction until no air leak remains
- Pleurovac contains no bubbles with respiration
- Do not apply a Heimlich Valve in cases of Trauma
- Use only for simple Spontaneous Pneumothorax in a patient going home
- References
- Majoewsky (2012) EM:RAPC3 2(1): 1-2
- Keep Chest Tube clamped until suction applied
- Testing for persistent air leak
- Ask patient to cough while observing Chest Tube output
- Water seal chamber OR
- Heimlich Valve immersed in water
- Air bubbling through water on coughing suggests persistent leak
- Continue to leave in Chest Tube until no persistent air leak is found
- Consider other causes of air leak (e.g. leaky vacuum tubing, Chest Tube hole not fully in chest)
- Ask patient to cough while observing Chest Tube output
- Chest Tube removal timing
- At least 24 hours after air leaks have stopped AND
- Chest Tube drainage <200 ml per 24 hours AND
- Serous drainage AND
- Not intubated on Ventilator or other form of Positive Pressure Ventilation (e.g. Bipap, CPaP)
VIII. Complications
- Typical complications (similar to any invasive procedure)
- Infection
- Empyema
- Chest wall Cellulitis
- Necrotizing Fasciitis
- Bleeding
- Intercostal Vessel or intrathoracic vessel disruption
- Scarring
- Infection
- Chest Tube specific complications
- Chest Tube malposition (most common)
- Tension Pneumothorax (if Chest Tube becomes obstructed)
- Blocked Chest Tube drain
- Chest Tube dislodgement
- Reexpansion Pulmonary Edema
- Subcutaneous Emphysema
- Chylothorax
- Persistent air leak
- Common concern when there is a persistent communication between Bronchioles and pleural space
- Consider other causes of air leak (e.g. leaky vacuum tubing, Chest Tube hole not fully in chest)
- Organ injury
- See precautions above
- Lung injury
- Nerve injury
- Great Vessel injury
- Liver injury (right)
- Spleen or Stomach injury (left)
IX. Resources
- Chest Tube Insertion (NEJM) - Part 1
- Chest Tube Insertion (NEJM) - Part 2
- Regions Trauma Professional's Blog (Michael McGonigal, MD) - Chest Tube insertion
X. References
- Swadron and Inaba in Herbert (2019) EM:Rap 19(6): 15
- Swanson (2019) Crit Dec Emerg Med 33(3): 12-3